civilsonya
sonya 时间:2021-01-11 阅读:()
RESEARCHARTICLEOpenAccessMoralexperiencesofhumanitarianhealthprofessionalscaringforpatientswhoaredyingorlikelytodieinahumanitariancrisisMatthewHunt1,2*,AniChénier3,KevinBezanson4,ElyséeNouvet5,CarrieBernard6,7,SonyadeLaat3,GauthamKrishnaraj3andLisaSchwartz8AbstractWars,disasters,andepidemicsaffectmillionsofindividualseveryyear.
Internationalnon-governmentalorganizationsrespondtomanyofthesecrisesandprovidehealthcareinsettingsrangingfromafieldhospitaldeployedafteranearthquake,toahealthclinicinalongstandingrefugeecamp,toatreatmentcenterduringaninfectiousdiseaseoutbreak.
Theprimaryfocusoftheseactivitiesistosavelives.
However,inevitably,manypatientscannotbesaved.
Weundertookaninterpretivedescriptionstudytoinvestigatehumanitarianpolicy-makerandcareproviders'experiencesandperceptionsofpalliativecareduringhumanitariancrises.
Inthispaper,wereportoninterviewswith23healthprofessionals,11ofwhomalsohadexperienceaspolicy-makerswithinahumanitarianorganization.
Weusetheconceptofmoralexperienceasananalyticlens:participants'experiencesofvaluesthattheyheldtobeimportantbeingrealizedorthwartedastheyrespondedtotheneedsofpatientswhoweredyingorlikelytodie.
Weidentifiedfivethemesrelatedtoparticipants'moralexperiences,allofwhichrelatetovaluesofcompassionintheprovisionofcare,andjusticeinaccessingit.
(1)Participantsdescribedinterveningtoeasethesufferingofdyingpatientsasaninherentaspectofhumanitarianismandtheirdutyashealthprofessionals.
(2)Participantsalsoexpressedthatupholdingdignitywasofcriticalimportance,stemmingfromarecognitionofsharedhumanityandasanactofrespect.
(3)Sincehumanitarianactionisprovidedinsituationsofscarcity,prioritizationisinescapable.
Acknowledgingtheprimacyofcurativecareinemergencies,participantsalsoemphasizedtheimportanceofensuringthatcareforthedyingwasattendedto,includingduringtriage.
(4)Participantsreportedworkingwithinandpushingagainstsystemicconstraintssuchaslegalorlogisticalbarrierstoopioids,lackofguidelines,andconflictingviewswithcolleagues.
(5)Giventhestakesinvolved,participantsfeltaheavyweightofresponsibilityanddescribedtheirchallengesincarryingit.
Thesefindingsilluminateexperiencesrespondingtopatientswhoaredyingorlikelytodie,andhowtheseconnectwiththevaluesofhumanitarianhealthprofessionals,sometimesresultingindissonancebetweenvaluesandactions.
Theyalsopointtotheneedtomakemorespaceforpalliative,alongsidecurative,approachestocareinsituationsofhumanitariancrises,ideallybyfurtherintegratingthem.
Keywords:Disaster,End-of-life,Epidemic,Ethics,Humanitariancrisis,Moralexperience,Non-governmentalorganizations,Palliativecare,Reliefwork,Values,War*Correspondence:matthew.
hunt@mcgill.
ca1SchoolofPhysicalandOccupationalTherapy,McGillUniversity,845SherbrookeStreetWest,Montreal,Quebec,Canada2CentreforInterdisciplinaryResearchonRehabilitation,Montreal,Quebec,CanadaFulllistofauthorinformationisavailableattheendofthearticleJournalofInternationalHumanitarianActionTheAuthor(s).
2018OpenAccessThisarticleisdistributedunderthetermsoftheCreativeCommonsAttribution4.
0InternationalLicense(http://creativecommons.
org/licenses/by/4.
0/),whichpermitsunrestricteduse,distribution,andreproductioninanymedium,providedyougiveappropriatecredittotheoriginalauthor(s)andthesource,providealinktotheCreativeCommonslicense,andindicateifchangesweremade.
Huntetal.
JournalofInternationalHumanitarianAction(2018)3:12https://doi.
org/10.
1186/s41018-018-0040-9IntroductionHumanitarianhealthcareaimstosaveandsafeguardthelivesofpeoplecaughtupinsituationsofcrisis.
Thisisenactedindiversesettings:internationalnon-governmentalorganizations(NGOs)implementvaccinationandfeedingprograms,setuptreatmentcentersduringoutbreaksofinfectiousdiseasessuchascholeraandEbola,providepri-marycareinrefugeecamps,andestablishfieldhospitalstodeliversurgicalcareduringwarsandfollowingnaturaldisasters,amongstmanyotheractions.
Despitethebestintentionsanddedicatedcareofhumanitarians,manypa-tientswilldieduetoinjuryorincurabledisease.
Thisisaninescapablereality,especiallygiventheprecarityandresourcescarcitythatcharacterizehumanitariancrises.
Theoverridingimperativeofsavinglivesinhumanitar-ianhealthcare,however,hasoftenleftlimitedroomforaddressingsufferinganddignity,especiallyforindivid-ualswhoaredying,inhumanitariansettings(Powelletal.
2017).
Therehasalsobeenalackofguidanceandsupportrelatedtocaringfordyingpatientsduringhu-manitariancrisis(Nouvetetal.
2018),asituationwhichmayincreaseuncertaintyandleadtomoraldistress.
Inthepastfewyears,increasedattentionhasbeendi-rectedtowardpalliativecareprovisionbyhumanitarianhealthprofessionals.
TheWorldHealthOrganization(WHO)definespalliativecareas"anapproachthatim-provesthequalityoflifeofpatients(adultsandchildren)andtheirfamilieswhoarefacingproblemsassociatedwithlife-threateningillness.
Itpreventsandrelievessuf-feringthroughtheearlyidentification,correctassess-mentandtreatmentofpainandotherproblems,whetherphysical,psychosocialorspiritual"(WHO2018).
Commentatorshavearguedfortheimportanceofpalliativecareprovisioninsituationsofwar,disaster,andepidemic(Marstonetal.
2015;SmithandAloudat2017),withPowelletal.
arguingthatitshouldbecon-sidered"anintegralcomponentofreliefstrategies"(2017:1498).
SomeNGOshaveestablishedpoliciestosupporttheirfieldteamsinprovidingcareforpatientswhoarenotexpectedtosurvive,suchastheInter-nationalCommitteeoftheRedCross'striageguidelineswhichidentifyminimumcarestandardsforthesepa-tients(GiannouandBaldan2009).
Broadereffortsthatcrossthehumanitarianfieldarealsounderway,includ-inganinitiativetointroduceanewchapterintheSphereHandbook:HumanitarianCharterandMinimumStan-dardsinHumanitarianResponseaddressing"reliefofsufferingandend-of-lifecare.
"1Evidence-basedstan-dardsforsupportivecareinEbolaTreatmentCentershavealsobeendevelopedandincluderecommendationsforpaincontrolandaddressingpsychologicaldistress(Lamontagneetal.
2018).
Theseinitiativeshavethepotentialtofurtherfore-groundtheneedforpalliativecareinhumanitariansettingsandestablishguidancetohelporientpractice.
Thereremains,however,littleinformationaboutpalliativecareinterventionscarriedoutaspartofthehumanitarianresponsetocrises(Schneideretal.
2017),includingexpe-riencesofpatients,families,andcareproviders.
Withthegoalofbetterunderstandingopportunities,obstacles,andexperiencesofpalliativecareprovisioninhumanitariancrises,wehaveundertakenamulti-stageresearchprojectthatincludesasurvey,interviewswithhumanitarianhealthprofessionalsandpolicy-makers,andin-depthcasestudies,includinginterviewswithpatients,families,andhealthprofessionalsinRwanda,Jordan,andGuinée(HumanitarianHealthEthicsResearchGroup2018).
Inthispaper,wefocusonexperiencesofprovidersofcareandreportoninterviewsweconductedwith23healthprofes-sionals,11ofwhomalsohadexperienceaspolicy-makerswithinhumanitarianNGOs.
Ouranalysisfocusesontheirmoralexperiences,thatissituationsinwhichtheyexpe-riencedvaluestheyheldtobeimportantasbeingrealizedorthwarted(HuntandCarnevale2011)astheyrespondedtotheneedsofpatientswhoweredyingorlikelytodieinahumanitariancrisis.
MethodsThisinquirywasguidedbyinterpretivedescriptionmeth-odology(Thorne2016)andwasundertakenwithinacon-structivistparadigminwhichhumanexperienceisunderstoodassubjective,local,sociallyandexperientiallybased,andculturallyandhistoricallyspecific(Lincolnetal.
2011).
Interpretivedescriptionaimstodevelopa"coherentconceptualdescriptionthattapsthematicpatternsandcommonalitiesbelievedtocharacterizethephenomenonthatisbeingstudiedandalsoac-countsfortheinevitableindividualvariationswithinthem"(Thorneetal.
2004:7).
Here,wereportonouranalysisoftheinterviewsan-sweringthefollowingquestion:"Whatarethemoralexpe-riencesofhumanitarianhealthprofessionalsastheyrespondtotheneedsofindividualswhoaredyingorlikelytodieduringahumanitariancrisis"Thisanalysisisguidedbythefollowingunderstandingofmoralexperi-ence:"Moralexperienceencompassesaperson'ssensethatvaluesthatheorshedeemsimportantarebeingreal-izedorthwartedineverydaylife.
Thisincludesaperson'sinterpretationsofalivedencounter,orasetofliveden-counters,thatfallonspectrumsofright-wrong,good-bad,orjust-unjust"(HuntandCarnevale2011:659).
Thus,inquiryintomoralexperienceaimstoilluminate"thelocalprocesses(collective,interpersonal,subjective)thatrealize(enact)valuesinordinaryliving"(Kleinman1999:71).
EthicsThisstudywasreviewedandapprovedbytheHamiltonIntegratedResearchEthicsBoardatMcMasterUniversity,Huntetal.
JournalofInternationalHumanitarianAction(2018)3:12Page2of13andtheMcGillFacultyofMedicine'sInstitutionalReviewBoard.
Allparticipantsprovidedwritteninformedconsenttoparticipateinthestudy.
RecruitmentWerecruitedparticipantsusingfourapproaches.
First,wedistributedinformationaboutthestudyonsocialmedia(viaourresearchgroup'sTwitterandFacebookaccounts).
Second,wesharedinformationwithinourprofessionalnetworkswhichresultedintherecruitmentof11participants.
Third,attheendofthesurveythatwasconductedbyourresearchteamaspartofthebroaderproject(seeElrha2017),weinvitedsurveyre-spondentstoindicatetheirinterestinalsoparticipatinginaninterview.
Nineparticipantswererecruitedthroughthesurvey.
Finally,werecruitedthreepartici-pantsusingsnowballsampling,askingintervieweestosuggestotherswhomightbeinterestedandeligibletoparticipateinthestudy.
Throughoutthisprocess,weattemptedtorecruitadiversegroupofparticipants,in-cludingmenandwomen,andindividualsaffiliatedwithdifferentorganizations,comingfromdifferentregionsoftheworld,andwithexperienceworkingindifferenthu-manitariansettingsandindifferentcapacities.
ParticipantsThispaperreportsontheanalysisofinterviewswith23healthprofessionals(16physicians,6nurses,andonephysicaltherapist),11ofwhomhadalsoworkedaspolicy-makerswithahumanitarianorganization.
Inthiscomponentofthestudy,wehadalsointerviewedanon-clinicianpolicy-makerbutthatinterviewisnotin-cludedintheanalysispresentedhereduetoourfocusonexperiencesofcareprovision.
The23participantswereaffiliatedwith18differentorganizationsandin-cluded11menand12women.
MostoftheparticipantshadworkedwithlargerinternationalorganizationsbasedinEuropeorNorthAmerica.
Ourpurposivesamplingwaslimitedinthatparticipantsincludedmorephysi-cians(16)thanotherhealthprofessionals(7)andmoreindividualsfromhigh-(19)thanlow-ormiddle-incomecountries(LMICs)(4).
InterviewsInterviewswereconductedbetweenNovember2016andMay2017,inEnglishorFrenchaccordingtotheprefer-enceoftheparticipant,andfollowedaninterviewguide.
Wecreatedtwoversionsoftheinterviewguide(oneforparticipantswhohadexperienceonlyasclinicians,andoneforparticipantswhoalsohadexperienceasapolicy-maker),andeachwasrefinedbasedonfeedbackfromexperiencedhumanitarianhealthprofessionalsandpolicy-makers,andpersonswithexpertiseinpalliativecare.
AllinterviewswereconductedbySkypeortelephoneduetothegeographicdispersionofthepartic-ipants.
Interviewsrangedfrom49to92mininduration(average65min).
AnalysisWeinitiatedtheanalysisoftheinterviewsastranscriptsbecameavailable.
InductivecodingwasdonebytwoteammembersandorganizedusingNVivosoftware.
Therewereseparatecodersforthepolicy-maker(GK)andhealthprofessional(AC)interviews.
Ateammember(MH)independentlycodedsectionsoffourtranscripts(twoforpolicy-makersandtwoforhealthprofessionals),andthreeteammembers(KB,CBandEN)independentlycodedonepolicy-makerinterview.
Theprovisionalcodebookwasrefinedthroughdiscussionwiththewholeteamandthroughcomparisonofcodedtranscripts.
Ananalyticstructurerelatedtomoralexperiencewasthendevelopedbythreeteammembers(MH,KB,andAC)byrepeatedandclosereadingofthetranscripts,useofvisualmatricesandconceptmaps,anddiscussion.
Onceaninitialanalyticstructurewasestablished,ateammember(MH)rereadalltranscriptsinlightofthisemerginganalysistotestitsconsistencyandcomprehensiveness.
Theanalyticstruc-turewasthenrevisedthroughteamdiscussion.
ResultsParticipantsdescribedanddiscussedexperiencesofpal-liativecareprovisionandreflectedonitsplaceinhu-manitarianresponse.
Usingthelensofmoralexperience,weanalyzednarrativesofcareinwhichparticipantsexperiencedvaluestheyheldtobeimportantasbeingrealizedorthwarted.
Manyvalueswereimplicatedinthesedescriptions.
Theyclusteredaroundtwounder-lyingcommitments:tojusticeinaccesstocareandcom-passioninprovisionofcare.
Throughaprocessofinductiveanalysis,weidentifiedfiveinterlinkingdimen-sionsofmoralexperienceinrelationtocaringforpa-tientswhoweredyingorlikelytodie:actingtoeasesuffering,upholdingdignity,balancingcarepriorities,workingwithinandresistingsystemicconstraints,andbearingtheweightofresponsibility.
Tworelatetowhatmanyunderstoodasimperatives:actingtoeasesuffer-ing,andupholdingandpreservingdignity.
Theotherthreerelatetoparticipants'experienceofworkingtomeettheseimperativesintheheavilyconstrainedcon-textofhumanitarianaction:balancingcarepriorities,workingwithinandresistingsystemicconstraints,andbearingtheweightofresponsibility.
Distinctyetcon-nectedintheunderlyingcommitmentstojusticeandcompassionthatinspiresandinformsthem,thesethemesshedlightonwhyandhowhealthprofessionalsengagedinhumanitariancrisesexperiencetheneedsforpalliativecareprovisionasmorallyimportant,some-timeshaunting,experiences.
Huntetal.
JournalofInternationalHumanitarianAction(2018)3:12Page3of13ActingtoeasesufferingOurparticipantsviewedactingtoeasesufferingasanintegralcomponentofgoodcareforallpatientsinhumanitariansettings,butespeciallyimportantforindivid-ualswhoaredyingorlikelytodie.
Theyalsodescribedhow,duetovariousfeaturesofwars,disasters,orepi-demics,thisdimensionofcaremaybeneglectedoreclipsedbyanoverwhelmingconcernforsavinglivesandstewardinglimitedresources.
Asaresult,andillustratedinmanyofthenarrativesrecountedbyparticipants,sufferingistooofteninsufficientlyaddressed,evenmoresoforpeoplewhoaredying.
Nonetheless,whencurativecarewasunavailableorinappropriate,participantsarguedthatpal-liativecareshouldbeprovidedandthataddressingsymp-tomsandrelievingpainwasanobligationofhumanitarianhealthprofessionals,andthatnotdoingsorepresentedaninjustice.
Aphysicianinvolvedindevelopinghumanitarianpalliativecareguidelinesarguedstronglyfortheimport-anceofalleviatingsuffering,since"notgivingpalliativecareandpaintreatmentisexactlylikenon-assistancetopersonsindangerorlikeacceptingtorture.
Becausesomepainsareliketorture"(P1).
Whilemakingtheseassertionsabouttheimportanceofalleviatingsuffering,participantsconsist-entlyexpressedthatlifesavingwastheprimaryfocusofhumanitarianhealthcare.
Generally,theyviewedalleviationofsuffering,includingfordyingpatients,assomethingthatwascompatiblewithandcomplementarytothisfocus.
Severallinkedthisclaimtothemandateofhumanitar-ianaction,since"ahumanitarianorganization…[has]avocationofcaringforthemostfragilepeopleintheworld"(P4).
Giventheextremevulnerabilityofindivid-ualswhoaredying,addressingtheirsufferingwasde-scribedasinherenttothevisionofhumanitarianaction.
Aphysicianinvolvedintrainingandpolicy-makingataninternationalNGOtookahistoricalperspective,statingthatpalliationwaspartofthe"DNA"(P10)ofhumani-tarianismasitwascentraltothefoundingoftheRedCrossmovementthroughtheactionsofHenriDunantattheBattleofSolferinoin1859.
Thisalignswiththeideasexpressedbyparticipantswhoemphasizedthateffortstoalleviatesufferingwereconsistentwith,andevenamountedtoareclaimingof,humanitarianvalues.
Inthissense,theseparticipantsfeltthathumanitariansfallshortoftheiridealsand"missthemark"(P17)iftheydonotaddresssuffering,especiallyofdyingpatients.
Anursewhohadtakenpartinthehumanitarianre-sponseafteranearthquakeandduringacivilwardescribedseveralsituationswhereshesoughttoaddresspatients'suffering,aswellascircumstanceswhendoingsowasespeciallydifficult.
Inherinterview,shefre-quentlyreturnedtoasituationwhereactivefightinginCentralAfricaledtoherteambeing"inundatedwithhundredsofpatients"(P19).
Sheassertedthatevenincircumstanceswhentriagingpatientswasunavoidable:…ifyoudon'tprovidesomethingforpain,andyoudon'tdothelittlethingsthen–thenyou'relosingalittlebitofwhyyou'reeventhereandthewholemoralpiecetoit…thehumanitarianpiece.
Otherwiseyou'rejustabunchofmedicsrunningaroundinthefield,tryingto…stopthebleeding,butwhen–ifyou'regonnabehumanitarians,thenyouhavetoreallylookatthathumanpiece…(P19)Highlightedactionstoalleviatesufferingincludednotonlyprovidinganalgesicsbutalsoprovidingwater,put-tingupasunshade,andhavingsomeonestaywithgrievouslyinjuredpatientswhoweretriagedtonotre-ceivelifesavingcare.
Failuretoengageinsuchacts,shefelt,wouldrepresenthumanitariansfailingtoliveuptotheirvalues.
Alongwithmasscasualtytriagesituations,careprovisionindiseaseoutbreakswasalsodiscussedbymanypartici-pantsasacontextwhereattentiontosufferingwasex-tremelychallenging,yetnecessary.
Whileafewstorieswererelatedtooutbreaksofcholeraorotherdiseases,mostweretoldaboutthe2014–15Ebolavirusdiseaseout-breakinWestAfricatowhichsevenoftheparticipantshadresponded.
Inthissetting,curativeoptionswerenotavailable.
Anursereported,"whenIstartedwehadlikea70%mortalityrate,sobasicallyallweweredoingwaspalliativecare,Imeanwewerejustmakingpeoplecom-fortable…attheendoftheirlives"(P11).
SeveralparticipantsdescribedsituationsinwhichEbolapatientsweredyingbutinfectioncontrolmeasuresimpededthealleviationofsuffering.
Theseconcernswereparticularlyacutewhenpatientswerebleedingandvomitingorhaddiarrhea.
AphysiciandescribedcominguponanEbolapatientwhowasimminentlydyingbutwhohadpulledoutherIVandtheneedlecouldnotbefound.
WhileencumberedbytheirPersonalProtectiveEquipment,shedescribedenteringtheroomwithacolleagueand:keepingsortofmybuddysafe…andfindingthesharp,that's,that'skindofwhathedidfirst,youknow,findingthehangingneedle…Ishouldhavetriedtoatleastmakehercomfortablewhileweweredoingthat,andI'mtryingtothinkofthetime,howmuchtimepassedbetweenusseeingherandherdyingand…itwaslike20minutes…soIthinkeven…duringthat20minuteswecould'vedonesomething.
Icouldhavethoughttodomoreorjustplannedbetter.
(P3)Sheexpressedregretthatshehadneitherattendedtothepatient'sdistressnorbeensufficientlyattentivetoherinthemomentofherdeath.
AphysicianwhohadcometoWestAfricafromanotherAfricancountrytoparticipateintheEbolaresponseHuntetal.
JournalofInternationalHumanitarianAction(2018)3:12Page4of13describedasituationwhenhefeltthatpalliativecarehadbeendoneespeciallywell:Yes,therewasthisboy,…[he]presentedtothe[EbolaTreatmentCenter],hehaddiarrheaandvomiting,and…whatwedidaspalliation,becausehediedeventually,wasIVfluids.
Irememberthatfluidsverywell,buthekeptstoolingandvomiting,andattimeswehadtogoinoneortwotimes,andusuallywegoinshifts,themorningshift,theafternoonandthenightshift,soatonepointweweregoinginmorefrequentlybecauseofhim.
Wedidalotoffluidresuscitation.
Hehadalotofabdominalpain,alotofabdominalpain,sowetriedtousealotofpainkillers.
Morphine,Tramadol,triedtouseallthat.
WhatelsedidwedoIthinkpsychosocialsupport…Andwhenwethinkthepatientswouldhavegivenuponlifeandthinkeverythingissobad,wewouldtrytosendthePsychosocialTeamtogotalktothem…AndIthink[that]particulardayhesortofdeteriorated,andbytheendofthedaywelosthim.
Therewereotherinstances,butthatwastheincidentthatittookmealongtimetotrytoforgetit.
(P5)Participantsalsospokeabouttheimportanceoffamily.
Manyrecognizedthatduringacrisis(anearthquakeoranepidemic,forexample)patientsthemselvesmayhavelostfamilymembersandbemourningtheirownlosses,andthatthelossoffamilymembersmaycompoundthefeelingofisolationduringtheirowndyingprocess.
ThiswasparticularlysoduringtheEbolaepidemicwhensomepatientshave"alreadylostyouknow10,15peopleintheirfamilies.
Everybodyhaslostsomebody"(P11).
Enablingpatientstoremainconnectedwithfamilywaspresentedasameanstoalleviatepsychologicaldistress.
Doingsowasdescribedasespeciallyvitalandchallen-ginginEbolaTreatmentCenters.
Suchactionsincludedbringingpatientstotheperimeterfencetointeractwithfamilymembers,orsupportingpatientsinisolationroomstocommunicatewithfamilyusingcellphonesortablets,orbyrecordingvideomessages(P20).
Eveninamasscasualtyemergency,aparticipantsuggestedtheimportanceofcreatingopportunitiesforrelativestobetogether(P14).
Attentiontosufferingwascloselyrelatedtoconcernforupholdingthedignityofdyingpatients,andthetwogoalswereoftendiscussedbyparticipantsasinter-twined.
Forexample,whenreplyingintheaffirmativethatprovidingpalliativecareshouldbeanobligationofhumanitarianorganizationsinemergencysituations,aphysicianlinkedsuffering,preservinghumanidentity,anddignifieddeath:"ifanybodyisdying,theyshoulddieasahumanandnotbelefttosuffer"and"Wherethere'sanemergencyandanybodydies,youshoulddieindignity"(P5).
Inthefollowingsection,weforegroundhowparticipantsdiscussedeffortstoupholdandpre-servehumandignity.
UpholdingdignityParticipantsconsistentlyemphasizedtheneedforhu-manitarianhealthprofessionalstoupholdthedignityofdyingpatients.
Theimportanceofdoingsowasde-scribedasstemmingfromarecognitionof,andresponseto,dyingindividuals'humanityandasanactofrespectandcompassion.
Inthislight,aphysicianexpressedthathumanitarianhealthcarerequired"strongpeoplewithstrongethics,butalsowithstrongcommitmenttovalueandtorespectthedignityofpeopleandothers"(P10).
Anotherphysicianexpressedthat"evenifapatientdoesnothavecurativesolutions",heorshe"isstillahumanbeing"andrequires"decentcarefordying"(P14).
Participantsdescribedmanyactionsasdignitypromot-ing,oneinparticularbeinghumantouch.
AphysicianreportedworkinginanEbolaTreatmentCenterwheretheteamplaceda"hugefocusonsortofattemptingtofocusondignity"includingensuringyoucan"safelytouchapersonandholdapersonandcleanaperson,youknow,whentheysoilthemselvesandsoforth"(P3).
Sheexpressedthatinanepidemic,itwascriticaltoseepatientsashumanbeings,notjustaspotentialtransmit-tersofdisease.
Anotherparticipant,anurse,describedthatevenwith50patientswhostillneededtobeseenbyherteam,itwasimportanttodemonstratecompassionand"holdachild,ortositandholdsomeone'shandorstroketheirback"(P21).
Suchactionsofhumanconnec-tionwerefrequentlyemphasizedbyparticipantsastheydiscussedtheimportanceofdignityfordyingpatients.
Akeyaspectofrespectingthehumanityofdyingpa-tients—andupholdingtheirdignity—wasensuringthattheydidnotfeelabandoned.
Referringtoadyingpatientwhomshehadwitnessedbeingplacedbehindashedbe-causetheclinicwasovercrowded,anurseasked,"whatisthehumanthingtodoPutting[dyingindividuals]behindtheshedandforgettingaboutthemisnottheanswer"(P19).
Leavingafellowhumanwithoutanycareandalonewhiletheyweredyingwasframedasbothaninjusticeandanindignity:AndIthinkalsoitprovidesthepatientwiththesenseofbeingcaredforuntiltheend.
Thatyouaren't…a'lostcause,'orthatyou'vebeen…'abandoned.
'Butthatyourlifestillmatterstotheveryend,however[much]timeyoudohave,andtolivewithasmuchcomfortaspossibleuntilthattime.
(P6)Aphysicianexpresseddismaythatinacrisis,dyingpa-tientswereputtothesideanddidnotreceiveattentionand"werealreadyconsidereddeadbeforetheyevenHuntetal.
JournalofInternationalHumanitarianAction(2018)3:12Page5of13died"(P23).
Incontrast,severalparticipantsdescribedtheimportanceofusing"presencewell"(P21)andenact-ing"accompaniment"(P4)fordyingpatients.
Accom-panimentalsoextendedtosupportingpatients'families;anursedescribedprovidingsupportforthemotherofaboywhohadaseverespinalcordinjuryafterfallingoutofatreeasanactof"help[ing]hismotherwalkthroughthiswholeissue"(P19).
Thevaluethatparticipantsplacedonensuringthatdyingpatientsfeelaccompaniedandnotabandonedisfurtherillustratedbythefollowingsituation.
Aphysicianrecountedwhyshehadagreedtopraywithapatientwhenthepatientaskedhertodoso.
Thoughde-scribingherselfasnotreligious,sheexpressedthatprayingwiththepatient"basicallysaidI'mwithyou"(P18).
Narra-tivessuchasthesemakevisiblethelinkinatleastsomehumanitarianhealthcareprofessionals'mindsbetweenrespondingtopalliativecareneedswithactivepresenceandacknowledgingacommonhumanity.
Dignitywasalsoassociatedwithaddressingconcernsre-latedtoprivacy.
Forexample,anursedescribedatlengthwhyshefeltthatprovidingprivacyforadyingpatientwascrucialforherdignity:"that'sahugepieceofittoo,like–notbeingondisplayforeverybody,sohavingprivacy,Ithink,whenyou'retalkingaboutwhat'simportantinpalliativecare,thedignityaspectishuge"(P19).
Shedis-cussed,however,thatitwasimportanttoconsiderthepossibilityofimposingnormsofprivacywithoutconsult-ingthepatient.
Indeed,treatingpatientswithrespectashumanbeingswasalsolinkedtoallowingpatientstovoicepreferencesandmakechoices.
Thehumanitariancontextsometimesmakesithardforpractitionerstofollowthisideal.
Anothernurse,reflectingonherexperiencesofthe2010Haitiearthquake,notedthatwith"cross-culturalandlanguagebarriers,sometimesthepatient'sopinionsandthoughtsjustaren'tgiventhetimeandweightthattheyoughttobegiven"(P21).
Amajorityofparticipantsemphasizedtheimportanceofpreserving"culturallyvalued"(P21)and"culturallyac-ceptable"(P7)endoflifepractices,acknowledgingthatwhatconstitutesdignityandadignifieddeathisnotthesameacrosstheworld.
Thisdiversitymayraisechal-lengesforhealthprofessionals,especiallyforexpatriates,includingaphysicianwhoexpressedtheimportanceofcaring"forthosewhomaynotsurviveandwhoalsodeservea,whateveryoudefinedignifiedas,adignifieddeath"(P6).
Theculturaldimensionsofdeathanddying—includingarounddignity—ledseveralpartici-pantstosuggestthatlocalhealthprofessionalswerebestplacedtoleadpalliativecareefforts.
Theyalsosuggestedthatlocalreligiousleaderswereimportantallies,andseveralgaveexamplesofworkingcollaborativelywithsuchindividuals.
AnAfricanphysician(P5)whohadrespondedtoahumanitariancrisisinaneighboringcountrywentfurtherandsuggestedthatpalliativecareeffortsshouldbecommunity-basedwithinternationalNGOs'roleslimitedtoprovidingoversightandsupport.
Effortstoupholddignityalsoextendedbeyonddeathandincludedfamilybereavement.
Participantsdescribedtheimportanceofmemorialsandfuneralservices,in-cludingaphysicianwhoexplainedthatshechosetoat-tendamemorialserviceasawayofhonoringpatientswhohaddied(P3).
InfectioncontrolduringEbolapre-sentedmanychallengesinthisregard.
Forexample,anursereportedthatwhiletraditionalpracticesofwash-ingthedeadbodywerenotallowedduetorisksofspreadingthevirus,theysoughtto"unzipthebodybagfor[thefamily]fromadistancesotheycansee,andhav-ingmoreattentiontokindofwhatthefuneralprocesslookedlike,andsothenwecould,atleastasmuchaspossible,honoreachperson"(P21).
Frominitialcontactuntilafterdeath,actionstoup-holdthedignityofpatientsfacingdeathwerefelttobecriticallyimportant,evenamidsttheinherentcomplex-itiesofresponse.
Throughactsofcaring,respondingtosuffering,upholdingprivacy,andrespectingtraditions,participantsexpressedthattheidentitiesandindividualworthofeachdyingpersoncouldberealized.
BalancingcareprioritiesEffortsaimedateasingsufferingandupholdingdignityareenactedinabroaderhumanitariancontext,oneinwhichresourcesarefiniteandoftenscarce,andlifesav-ingremainstheprimaryfocus.
Asnotedabove,partici-pantsacceptedthisbroadunderstandingofpriorities.
Forexample,aparticipantexpressedthatinthecontextofthewarinSyria,"thosepatientswiththepalliativeneeds,unfortunately…theystarttofeelliketheyaresec-ondpriority"(P16).
AmoreextremeversionofthisprioritizationwasdescribedbyaparticipantinamasscasualtysituationfollowingviolentclashesinCentralAf-rica:"there'ssomanythatstillneedyourattentionthatwereallyhavenothingtoevenoffertothosethatwerenotgonnamakeit"(P19).
Anursestatedthat:Imean,obviouslyinabigdisaster,inabigmasscasualtyeventorareally,really,busycomplexconflict,theamountoftimethatpeopleareabletogivetopalliativepatientsisgoingtobelimited.
AndIthinkthat,unfortunately,that'sareasonabledecision…(P23)Whileacknowledgingtheneedtoprioritizelifesaving,severalparticipantsnonethelessdescribedtheprovisionofcaretodyingpatientsasanessentialobligationofjustice.
Aphysicianwhohadexperienceasapolicy-makerdescribeditthus:"…patientswhosimplyneeddecentcarefordying-youneed,youareobligedtocalculateandprovidere-sourcestoaccommodatethosepatients….
"(P14).
GivenHuntetal.
JournalofInternationalHumanitarianAction(2018)3:12Page6of13thesecommitments,participantssuggestedthathumanitar-ianhealthprofessionalsshouldmakeprovisionstoensurethatsuchcareispossible.
Forexample,anotherphysicianpolicy-makerrecommendedthatsomehealthcareresourcesshouldbededicatedtoaddressthesufferingofdyingpa-tientsevenduringtriagesituations,includingreservingpainmedicationforthesepatientsand:tokeepsomeresourceevensomepartofthe,ofthestaff…topayattentionandtoprovidethisbasiccaretopeoplewhowillnotbereceiving…life-savingtreatment:theywillprobablydie,theymaydie,butatleasttheyshoulddie…inarespectfulway,inadignifiedway,andasmuchaspossiblewithouttoomuchpainandwiththepresenceofsomebody.
(P10)Severalparticipantsexpressedthatitisimportantnottoextrapolatefromthemostacutesituationsofurgencyasarationalefornotaddressingsufferingorpromotingdignityforpatientsinotherhumanitariansettings.
Astheacuityofanemergencydecreases,aphysiciannotedthattherationaletolimithealthcaretoprimarilylifesav-ingefforts,withlimitedattentionavailabletorespondtootherneeds,"doesn'tstaytrue"(P18).
Moreover,adistinc-tionwasdrawnbetweenbasiccarethatattendstosuffer-inganddignityandamorecomprehensiveversionofpalliativecare,whichsomesawas"aluxury"(P2,P11)inacutehumanitariansettings.
Fundamentally,participantshighlightedwhattheysawasafalsedivideandtheneedformoreintegrationofcura-tiveandpalliativeapproaches.
Addressingthepossibilitythatthefocusonlifesavingwouldnotleaveroomforpalliativecareapproaches,aparticipantthuscalledforhu-manitarianstorejectachoicebetweenpalliativecareandcurativecare.
Heexpressedthathumanitariansshouldprovidelifesavingcareand"simultaneously…providees-sential,basichumancareto[patientswhowilldie].
Andit'snotoneortheother.
It'sweneedtocombinebothapproaches,andthisprobablyisasmallrevolutioninthewayweenvisageourroleinthefield.
"(P10).
Workingwithin,andresisting,systemicconstraintsParticipants'effortstoprovidepalliativecarewerecir-cumscribedbysystemicconstraintsinherenttohumani-tarianoperationsandtothewidercontextofglobalinequalityinhealthcareaccess.
Participantsidentifiedthedifferentwaysinwhichtheyengagedwithunfairsys-tems,andtheimpactthesedifferentwaysofengaginghadonthecaretheyprovidedpatients,andontheirownwell-beingascareproviders.
Participantsempha-sizedthatitwasfeasibletoaddressmanyneedsofdyingpatientsinhumanitariansettings.
Aphysicianwhohadworkedinthreesituationsofarmedconflictstatedthat"…fromahumancompassionperspective,somethingsthatpeopledieofarepainfulanduncomfortable.
Andwehavethetoolstolimitthatdiscomfortandweshouldusethem"(P23).
Variousfeaturesofhumanitarianpro-jectswereidentifiedasenablingsuchcare,includingstrongpartnershipswithlocalorganizations,havingclearguidanceandsupportiveleadership,andaccesstoopi-oidsandotherneededresources.
However,itwasmorecommonforsystemicfeaturesandarangeofbarrierstoconstrainhealthprofessionalsintheirresponsetothosewhoweredyingorlikelytodie.
Forexample,careop-tionsareoftenlimitedbylackofaccesstomaterialandhumanresources.
Participantsdescribedlackofaccesstopainmedications,especiallyopiates,aswellasequip-ment(e.
g.
,diagnostics,ventilators)andsupplies.
Short-agesofstaffwithskillsandtraininginpalliativecareorthepresenceofstaffwithskepticalorcontraryviews(betheylocalorexpatriatehealthprofessionals)werealsohighlightedasbarriers.
Whencoupledwithalackofclearpalliativecareorganizationalpolicyguidanceandclinicalguidelines,theseobstacleswerefurtherrein-forced.
Othersystemicfeatureswerealsoidentified.
Participantswereconcernedwhentheysawpatternsofneglectingsuffering.
Forexample,aphysicianfeltthatthistendencyreflecteda"tyrannyoflowexpectations"(P22)whichsheassociatedwithaformofimplicitra-cismandwhichresultedinhumanitarianorganizationsrespondinginadequatelytopainandsuffering.
Overall,participantsstressedthatthesechallengescanandshouldbeaddressedwithsustainedefforttoimproveaccessandthequalityofpalliativecareavailable.
Participantsframedmanyofthesefeaturesasunfairandasresultingfromand/orcontributingtowiderin-equalities.
Theydescribedcircumstancesasunjustatthegloballevel,suchasinequalitiesrelatedtowhichnationsbearthebruntoftheglobalrefugeecrisis(relativetotheirwealthandinfluence),orwhetheraparticularpatientwouldhavesurvivedtheirinjuriesiftheyhadoc-curredintheparticipant'shigherresourcedhomecoun-try.
Whilediscussingapatientwhodiedofaninfectedwound,aphysicianfromahigh-incomecountrynotedthat"Ithinkwefounditchallengingbecause…ifwe'dseenthisguypre-hospitalanywherein[homecountry],wewouldhavebeenabletodealwithlotsoftheseissuesquiteeffectively"(P17).
Anotherphysiciandescribedherdistress"performingtreatmentsthatIknewIcoulddowithlesspainandbettertolerabilityinabettersetting,butwasunabletodoatthattime"(P22).
Participantsalsodiscussedunfairnessinparticularcir-cumstances,suchasexpressingfrustrationwhenencoun-teringpatientsdyingfromconditionsthatcouldhavebeeneasilypreventedwithbetteraccesstobasichealthcare,andunfairnesswhencertainsubgroupswithinthelocalpopula-tionhadlessaccesstocare.
Severalparticipantsalsoidenti-fiedinequalitiesorinequitiesacrosshumanitarianprojects.
Huntetal.
JournalofInternationalHumanitarianAction(2018)3:12Page7of13Forexample,aphysiciandescribedhowtherewas"anunevensupplyofmedicationsacross"(P3)EbolaTreatmentCenters,includingmorphine.
Discussingthesamesitu-ation,anurseidentifiedthesourceoftheseinequalitiesasdifferentrulesamongsttheEbolaTreatmentCentersfun-dersandpartneringorganizations.
Sheworkedinacenterwheretherulesofapartneringorganizationprohibitedtheuseofmorphineandexpressedthat,asaresult,"therewasalotoffrustrationthatthingswerereallybadforthepa-tientsinourtreatmentcenters,andunfairlyso"(P21).
Participantsrespondedinavarietyofwaystosystemicconstraintsandtheinequalitiesandunfairnessthattheyengendered.
Insomesettings,participantsfelttheyneededtomakereasonableifdifficultcompromisesduetotheconstrainingnatureofthecircumstances.
Work-inginaninsecureandchaoticarmedconflictsettingwheretherewerefewhealthprofessionals,aphysicianreportedreluctantlymakingthedecisiontonotallowfamilytovisittheirdyinglovedonesinthehospital.
Theteamwas,however,abletoprovidepainmanagementdespitethelimitednumberofhealthcarestaff:Thesepeoplemaydiewithouttheirfamilymembersaroundthem,whichisobviouslynotideal.
Butinthosecases,Idothinkthat'sareasonablelimittotakeforsecurityreasons,forresourcereasons,forfunctionofthehospitalreasons.
So,thatwouldbeacompromisethat'smade,suboptimalstaffing,perhaps,andsuboptimalpsychosocialcare,butnevertheless,abasicminimumintermsofpainmanagement.
(P23)Participantsalsodescribedthattheyandtheircol-leaguessometimesneededtoadjusttheirperspectiveinhumanitariansettings.
AphysicianfromNorthAmericaexpressedthatexpatriatehealthprofessionalsneedtoaccept"thatwecan'tdotherewhatwecando[inhomecountry]"(P15).
Shealsodescribedhowshehadneededtolearntobecomemoreacceptingofthedecisionsmadebypatientsandtheirfamilies.
Shereportedthatitwasdifficultforhertounderstandamother'sdecisionprocess:wecan'tevenconceiveofit,wecan'tevensortouthowshe'smakingherdecisions,ifshe'sgoingtostaywiththatchild[inthehospital]orshe'sgoingtogohomeandlookaftertheothereightonesthatdon'thaveanybodylookingafterthembecausetheirDadhasalreadybeenkilledinthewar.
(P15)Humanitarianhealthprofessionalsreacttothesediffi-cultiesinvariedways,sometimesgoingbeyondadjustingperspectives,tolosingperspective.
Aphysicianreportedthattheaustereanddifficultcircumstancesofhumani-tarianemergenciescanleadexpatriatehealthprofessionalsto"turnpeopleinto'other',turnoffyouremotionsandjustbelike,'holdthemdownandwe'lldothis'"(P22).
Sheassertedthattakingthisperspectivemustbeactivelyresisted;regardlessofthecircumstancesinwhichpeopleareliving,theyshouldbetreatedwithrespectandbepro-videdcaretorelievetheirsuffering.
StoriesofresponsivenessandadaptationinthecontextoftheWestAfricanEbolaepidemic,forexample,high-lightwaysthatteamsbecamemoreadeptatworkingwithinandpushingagainstconstraints,includingbychallengingpoliciesandinnovatingtobetteraddressneedsofpatientsinacontextofextremelyhighmortal-ityrates.
Aparticipantdescribedthathisteam"gotalotbraverandalotmoreboldwithhowweweretreatingpeopleandgivingthemalotmoreattentionoralotbet-tercare"(P11)astheEbolaoutbreakprogressedandtheydevelopedmoreknowledgeandskillformanaginginfectioncontrolriskswhileprovidingbetterandmorecompassionatecaretopatients.
Inothersettings,emer-genttechnologieswereidentifiedasprovidingsupporttoovercomeobstaclestocare.
Forexample,telemedicinewasidentifiedbytwoparticipantsasameanstoaccessexpertsinpalliativecareinsituationswheretheteamlackedsuchexpertise.
Inanothercontext,aphysiciandescribedhow,evenwhenopioidswerenotavailable,ultrasound-guidednerveblockscouldbeusedtoprovideeffectivepainrelief.
Advocacywasalsodescribedasanimportantpositiveresponsetoobstaclesandconstraints.
Thismightoccuratmultiplelevels:withintheteam,intheorganization,andinternationally.
Aphysicianpolicy-makerexpressedthathumanitariansshould"advocate.
.
.
forpalliativecareinhumanitariancrisestobeabasichumanright…Itshouldbethenorm.
Itshouldbeahumanrightandthenorm"(P1).
Manyparticipantssuggestedthathumani-tarianscanadvocatewithintheirorganizationforbetteraccesstoresourcesneededforimprovingbothcurativeandpalliativecare.
Aphysicianexpressedthatthesedualadvocacyeffortsgo"hand-in-hand"(P3).
Discussingthemanyburnedpatientsforwhomherteamwasunabletoprovideadequatepainmedication,aphysicianexpressedregretthatshehadnotbeenmoreforcefulinheradvo-cacyefforts,sayingthat"IfIhadbeenalittlebitmoreontheballaboutit,Icouldhavekickedupabiggerstink"anddemandedmorphineandketaminebemadeavailable(P22).
Thesevariousresponsesultimatelyre-flecttheweightofresponsibilityandmoralobligationparticipantsexperiencedinhowtheyrespondedtopa-tientsintheircarewhoweredying.
BearingtheweightofresponsibilityThenarrativesconveyaprofoundweightofresponsibil-ityfeltbytheparticipants.
Instoriesofpalliativecare"donewell"inahumanitariansetting,thisweightfeltHuntetal.
JournalofInternationalHumanitarianAction(2018)3:12Page8of13liftedoratleastlighterontheshouldersofparticipants.
Manyparticipantscouldnotthinkofacasewherepal-liativecarewasdonewell,butamongstthosewhocould,theirexperiencewasasourceofdeepsatisfaction.
Pro-vidingeffectivepalliativecare"…allowsthehealthcareworkerstofeelthattheyarecontributingandtheyhaven'tfailed"(P6).
However,evenwhencarewasdonewell,theseencounterscouldstillhauntparticipantsasmorallyandexistentiallysignificant.
Forexample,anursewhohadworkedinanEbolaTreatmentCentredescribed"alittlegirl,Ithinkabouttheageofnine,andwhocalledme,'Unclecanyouholdmyhand',andbe-causeIknewthatwecouldsitdownandtalktothem,so–whichIdid,andonceIheldherhand,shedied…andso,for-formany,manymonths,evenwhenIcame[home],Icouldstillfeelthattouch…Icouldstillfeel-hearthatvoice"(P20).
Thisexperiencestayedwithhim,andhedescribeditasonefactorinhisseekingpsycho-logicalsupportafterreturningfromhisfieldmission.
Situationswhichparticipantscharacterizedascarenotdonewellwereoftenassociatedwithparticularlyheavyemotionalstrain.
Somedescribedfeelingsofhavingfailedcertainpatients,andthesesituationsgaverisetodistressandfeelingsofguiltorregret.
Thisresponsewasparticularlyacutewhenparticipantsfeltthattheywereimplicatedinasituationthatwasprofoundlyandin-escapablyunjust.
Forexample,aphysiciandescribedhow"I'veliterallywatchedhundredsofbabiesseizetodeathandit'sjustaterrible…ButIdidn'thaveawayofkeepingthemcomfortable,andlettingthemdieinawarm,comfortableplaceandthatreallyhauntsme"(P22).
Feelingsomehowcomplicitinwhatwasoccur-ring,shewentontosaythat"Idon'tbelieveinhell,butIkindofthinkthereisaspecialplaceinhellforme.
"Especiallydifficultwerecircumstanceswhenpatientswhoweredyinginpainwereturnedawayfromcare,asituationwhichcanbe"devastatingemotionally"(P10)forhumanitarianworkers:"…itgoesagainsteverythingthatyou–asahealthcareworker,asahumanitarian,everything–todothattoahumanbeing,youknowthey'renotgonnamakeitandjustputthemaside,itwas–terrible(P19).
"Inadditiontostoriesofnotprovidingcaretodyingpatientsorofinsufficientlyaddressingsymptomsordig-nityfordyingpatients,participantsalsoreporteddistressaboutprovidingtreatmentthatprolongedthesufferingofadyingpatientwhentheparticipantfeltthatcareshouldhavebeenfocusedonpalliationbutwasnot,duetosecurityconcerns,orattheinsistenceofthefamilyorotherhealthcareprofessionals.
Participantsdescribedstrategiesthathelpedthemcarrytheweightofresponsibility.
Theyemphasizedtheimportanceofsharingtheweightwithtrustedcol-leagues,throughdiscussionandcollaborationwithinteams.
Closeteamrelationshipsthatincludedsharedplansforrespondingtotheneedsforpalliationwerede-scribedasimportant.
Aphysiciandescribedhowasharedplanallowedhisteamtofeel"comfortablewithwhateverwasgoingtohappen"(P15).
Otherstalkedaboutredirectingtheirfeelingsofnothavingprovidedsufficientcaretosomepatientsintoactionaimedathelpingotherpatients,includingthroughadvocacy.
Incontrast,severalparticipantsdescribedactivelytryingtoforgetcertaintroublingexperiences.
Organizationalstrategiesincludingsupportanddebriefingwerealsoidentifiedasvaluable.
Anursedescribedthelackofongoingpsychologicalsupportforhealthprofes-sionals,especiallynationalstaff,providingcareinEbolaTreatmentCentersasoneofthe"bigfails"ofhisorganization(P11).
Healsoidentifiedtrainingpriortodepartureasanimportantcomponentforhelpingpeopleanticipatethechallengesoffacingsuffer-ing,dying,anddeath,andbetterpreparingforthem.
Severalparticipantsreportedstrugglingwiththeirexperiencesofprovidingornotprovidingcaretodyingpatientsinahumanitariancrisis,evenaftertheirreturnhome.
Forexample,anursewhohadrespondedtotheEbolaoutbreakstatedthat:yes,itwasheavy…[S]omeofthethingsIdid,theydidn'tactuallycauseanyproblemswhileIwasthere,butwhenIcame[home],Icouldn'tsleep.
Itaffectedmysleep,myeating,evengoingtowalk.
Icouldn'thaveashowerforsometimesoitwasheavywhenIcameback…Ihadtoreceive–Igotsupport…psychotherapy,forIthinkupto6monthsor8months…(P20)Anotherparticipantreportedasimilarpattern,statingthat:Youthinkaboutthemwhenyoucome[home].
Youdon'thavetimetoprocessanything[inthefield],becauseyou–you'resooverwhelmedbythesituation,youdowhatyoucaninthatmoment,andyouhavetomoveon,becausethenextdaycouldbringtheexactsamething.
Soyoucanonlyprocessforyourownmentalhealthwhat'srightinfrontofyou.
Untilyoucomehome,atleast…andthenyoustarttokindof–reallythinkaboutwhatyoudid,orwhatyoudidn'tdo,and–sometimesthere'sabig–…discordanceofwhat–yourideals,andwhatyouactuallydid…theyjustaren'tmeetingupandit'sahugementalstrugglethen.
(P19)Fortheseparticipants,theweightofresponsibilitydidnotliftaftertheyreturnedtotheirhomecountries.
TheyreportedlingeringimpactsoftheseexperiencesofHuntetal.
JournalofInternationalHumanitarianAction(2018)3:12Page9of13respondingtotheneedsofpatientswhoweredyingorlikelytodieinhumanitariancrises,orofbeingunabletorespondtotheseneedsinwhattheyfeltwastherightway.
DiscussionParticipantsinourstudydescribedalleviatingsuffering,upholdingdignity,andaccompanyingindividualswhoaredyingorlikelytodieasobligationsofhumanitarianhealthprofessionalsandhumanitarianorganizations.
Notprovidingcaretosuchindividualsinhumanitariancriseswasdescribedandexperiencedbythemajorityasethicallywrong.
Atthesametime,seekingtoprovidepalliativecarefordyingpatientswaschallenging.
Inten-tionstoprovidesuchcarecouldbeseverelyconstrainedbylimitedresourcesavailableinthefieldorataparticu-larmomentinacrisis.
Thedominantethicofprioritiz-inglifesavinginthefaceoflimitedresourcesreinforcedlimitedpreparednessforandallocationofhealthcareresourcestowardthosepatientswhowerenotexpectedtosurvive.
Anawarenessofculturaldifferencesinend-of-lifepractices,expectations,andnorms(Gaudioetal.
2013;Gyselsetal.
2011;Hajjaretal.
2015)addedanotherlayerofcomplexitytothematterforprovidersworkingasexpatriatesincrisissettings.
Weproposethesescenariosanddecisionscameacrossasethicallytroublingtoparticipantsbecauseofthedegreeofsuffer-ingexperiencedbydyingpatients,butalsobecauseofthewaythesesituationshighlightedexistinglimitsforhealthprofessionalsrespondinginsituationsofhumani-tariancrisis.
Respondingtotheneedsofdyingpatientsinhumani-tariancrisesisheavilyfreightedwithethicalimplications,especiallygiventhepossibilityofdiscordancebetweenhumanitarians'valuesandwhatactionsseempossibleinahumanitariancrisis,arealitythatDeWaal(2010)hasdescribedasthetragedyofhumanitarianaction.
Thesesituationsalsointersectwithideasaboutwhatitmeanstobeahumanitarian,thedutiesofhealthprofessionals,andevenwhatitmeanstobeahumanbeing.
Encoun-terswithpatientswhoarelastinlinewithinatriagesystemthatprioritizestherescueandprotectionoflifearerememberedwithasenseofparticularimportance.
Forafewparticipants,decidingtoreservescarcehealth-careresourcesforthosepatientswhoareexpectedtosurviveaffirmstheirhumanitarianidentityandresponsi-bility,assuchdecisionslinktotheweightofhavingtodeterminehowtoallocatescarceresources.
Formost,suchchoicesleftparticipantsdeeplytroubled.
Expressedasguilt,outrage,ordistress,thesefeelingsarethemoralresidue(WebsterandBaylis2000)ofbeinginvolvedincompromisedcarethatgratesagainsttheirsenseofdoingthe"right"or"human"thingandpotentiallyresultinmoraldistress(Jameton1993).
Themoralworldsofhumanitarianhealthcareprofes-sionalsofwhichwecaughtaglimpsethroughthisstudyreflectandreaffirmthegoalsofhumanitarianactiontosavelives,alleviatesuffering,andmaintainhumandignity(SphereProject2011a).
Accordingtoourparticipants,thereluctancetoincludepalliativecareinhumanitarianhealthcareistheresultoftheoverarchingfocusonlifesav-ingandrescueinthiscontext,aviewwhichequatesdeathas(always)ahumanitarianfailure.
Recentcommentatorshavepushedforacceptancethatnotallpatientscanbesavedinhumanitariansettingsandthatthefailureliesinnottakingstepstoaddresssufferinganddignityforthosewhowillsuccumbtoinjuryordiseaseintheseset-tings(SmithandAloudat2017).
Participantsgenerallyexpressedhopethatmorecouldbedonefordyingpatientsinhumanitariancrises,inparticularbyinte-gratingcurativeandpalliativeapproachestocare,whilealsoacknowledgingsystemicandculturalchallengestodoingso(Huntetal,2017).
Theseconddraftoftheup-datedSpherehandbookendorsestheneedtoaddresssuf-feringandpainreliefforallpatients,includingpeoplewhoareexpectedtodie,andadvocatesforintegrationofpalliativeandcurativeapproaches(SphereProject2017).
Alongwithjusticeinaccesstocare,compassionstandsoutasanunderlyingethicalcommitmentinthepartici-pants'narrativesofcaringforpatientswhoaredyingorlikelytodie.
Whileitcouldbearguedthatallcareis(orshouldbe)compassionate,anumberofactionswereidentifiedbyparticipantsasmeaningfulmomentsbe-causeofthewaythesebroughtanon-medical,relationalcommunionwithpainandrecognitionofsharedhuman-ityintothehumanitarianpalliativesetting.
Thesein-cludedtouch,simpleconversation,andsharedprayerswithpatientsinthemomentspriortodeath.
Fundamen-tally,participantsappearedtoidentifywiththeuniver-salityofthehumanconditionsofpain,suffering,anddeath,andfeltitdemandedanempathetic,holistic,andtangibleresponse.
Itisinthisrecognitionandresponsetothehumanityoftheotherthatcompassionappearstoconnecttotheupholdingofdignityinparticipants'moralworlds.
Theconceptofdignityiswidelyusedinarangeoffields,yetitsdefinitionremainscontested.
Indeed,somebioethicsscholarshavearguedthatitisreplaceablebymorepreciseconceptssuchasrespectforpersonsandautonomy,evencallingita"uselesscon-cept"(Macklin2003).
Barclay(2018)hascounteredthisview,drawingonscholarshipfrompoliticalphilosophy,tosuggestthatthedistinctivecontributionofdignityisinemphasizingandembodyingequalmoralworth.
Thisperspectiveappearsconsistentwithourparticipants'useoftheterm,andtheiremphasisondignifieddeath,inclu-dingdyingpatientsnotfeelingabandonedortreatedaslessthanhuman.
Thisperspectivereflectsarelationalqualityofdignity.
ItisalsoresonantwiththebroaderHuntetal.
JournalofInternationalHumanitarianAction(2018)3:12Page10of13discussionofdignityinhumanitarianaction,whereitisdirectlyassociatedwithactsofrespectforpersonsaffectedbycrises(SphereProject2011b),andwithconceptionsofUbuntuinAfricanethicalthought(Behrens2013).
Behindthenarrativesofsomeparticipantswasacon-cernwithentanglementinsituationsofpoliticalandsocialinjustice.
Inthissense,providingpalliativecare,"becausethereisnothingelsetooffer,"isassociatedwithquestionsaboutbeingentangledinthemanufacturedcircumstancesthatprecipitatedsufferinganddeath.
Itreflectsabroaderconcernforaidworkerswho,adheringtothehumanitarianprincipleofneutrality,areconsciousthatadvocatingagainstinjusticecouldmeantheyloseaccesstothecommunityandthosewhoneedcaremost(Terry2002).
Differentformsofcomplicityinhumani-tarianactionhavebeenidentified,andattentionhasbeendirectedtodistinguishingthemfromrelatedethicalconcepts(LeporaandGoodin2013).
Amongstourpar-ticipants,severalexperiencedfeelingsofbeingcomplicitonamoreindividuallevel.
Participantsdescribedmo-mentswhentheyortheircolleaguesfailedtodoenoughasthemomentsthatcontinuetohauntthem.
Forex-ample,participants3and5expressedadeepandlinger-ingremorseforpatientswhotheyfeltweredeniedadignifieddeath,asahuman,duetoinactionontheirpart.
Theymayhavebeenunabletotakeamomenttospeakwiththepatient,toholdtheirhand,ortellthemwhatwashappening.
Feelingsofhavingfailedtoad-equatelyattendtopatientswithpalliativeneedsinhumanitariancontextsengendermoralstressthatturnsintomoraldistresswhenthecasesarecompounded,andindividualsfeeltheyhavecompromisedsignificantper-sonalandprofessionalvalues.
Lingeringeffectsofthissenseofcomplicityremainwithactorsasmoralresiduewhichmight,inturn,causethemtofeelhelpless,dis-trusttheirownactions,and,turnedinward,leadtocom-passionfatigueandburnout(Horningetal.
2017).
Thestudyfindingsalsodrawattentiontotheimport-anceoftrainingandpreparationintheareaofpalliativecareinhumanitariansettings.
Toeffectivelyrespondtotheneedsofdyingpatients,humanitarianhealthcareprofessionalsrequiretrainingandskills,aswellasguid-anceonhowtoprovidepalliativecareinhumanitariancrisissettings.
Ourparticipantsidentifiedexperienceswithpatientsandfamiliesfacingdyinganddeathasdeeplyaffecting.
However,manydescribedfeelingillequippedorunsupportedtorespondeffectivelytotheneedsofthesepatients,andthemoraldistressthiscreatedforthematthetime,andoftenlongafter.
Thisincludedseveralforwhomtheirexperiencesimpactedtheirmentalandemotionalwell-beingtoanextentthatmayhavejeopardizedtheirabilitytocontinueinhu-manitarianwork.
Formostparticipants,expressionsoftheethicalim-perativesofrespondingtosufferingandupholdingdignitywerealmostalwayscoupledwitharecognitionofthepragmaticneedfororganizationalandoperationalinclusionfortheresponsetobeconsistentandeffective.
Currently,thereareseveralongoinginitiativesthatareseekingtoaddressgapsintrainingandguidance.
Forexample,MédecinsSansFrontièreshasdevelopedapediatricpalliativecareguideline(SmithandAloudat2017)andMédecinsDuMondeisimplementingapilotprojectonpediatricpalliativecareintheDemocraticRepublicoftheCongo(seeMédecinsduMonde2016).
Theseareencouragingdevelopmentsandmoveindirec-tionsproposedbyparticipantswhoidentifiedorganizationaleffortstobuildaspaceforinclusionofpalliativecareases-sentialforengagingthecomplexcontextualissuesauthen-ticallyandconsistently.
Thecontextofhumanitariancrisescreatedneedsfortriageandprioritizingcarethatwereoftenunique.
Further,therewasrecognitionthatorganizationalpalliativecarestandardswouldrequiresignificantadaptationtolocalperspectivesgiventheculturalspecificitiesofthenatureofsufferinganddeath.
Differencesbetweenlocalandexpatriatepro-viders'viewsonsufferingorwhenandhowtoacknow-ledgetreatmentfutilitywerefrequentlycited.
Itwasalsorecognizedthatcareforthosefacingdeathwouldneedtoincludefamiliesandcommunitiesexplicitly.
Furthermore,differentformsofhumanitariancrises(e.
g.
,conflict,suddenonsetdisaster,epidemic)willshapeneedsandpossibilitiesforpalliativecareprovision,andthesedifferencesshouldbeaccountedforinguidelinesandtraining.
Onahigherlevel,itwashopedthatinclusionwouldalsobereflectedineffortsbythewiderhumanitariancommunitytoadvocateonissuessuchasaccesstoessentialpalliativemedicinesespeciallyopiatesandtheinternationalandnationalregulatoryandpolicyissuesthatarise.
AccordingtotheWorldHealthOrganization,"onlyabout14%ofpeoplewhoneedpalliativecarecur-rentlyreceiveit"(WHO2018).
Despiteglobalstatementsthatpalliativecareisahumanright(InternationalChil-dren'sPalliativeCareNetwork2008,WHO2018)andacorecomponentofuniversalhealthcoverage(WHO2018),accesstosufficientpainreliefisdeplorablylowinLMICs,especiallyamongstchildren(Knauletal.
2018).
ThisbackgroundsituationdirectlyaffectsaccesstopainmanagementinhumanitariancrisesinLMICs,especiallywherelaworpolicylimitorpreventtheimportationofopioids.
Humanitarianactorshaveexpressedacommit-menttoadvocate(NickersonandAttaran2012)andrallyinternationalorganizations,governments,policy-makers,andhealthcareproviderstotakethe"necessarystepstoensurethatallpatientsinneedhaveaccessto"essentialmedicinesforpalliativecare(DeLimaetal.
2007).
ItwasHuntetal.
JournalofInternationalHumanitarianAction(2018)3:12Page11of13feltthatadvocacybyhumanitarianproviderswouldfur-thertherecognitionandinclusionofpalliativecareinna-tionalandlocalhealthsystemsglobally.
Concernswereraisedaboutintroducingcarethatcouldnotbesustainedoncehumanitarianresponsehasended,butthiswasoffsetwiththepotentialopportunityforcapacitybuildingandhealthsystemsstrengthening.
Inresponsetotheirexperiencesinhumanitariancaresettings,manyofourparticipantswereledtoadvocateatdifferentlevelsfortheexplicitinclusionofpalliativecareinhumanitarianresponse.
Atthesametime,itiscrucialtoensurethatpalliativecareisnotseenasareplacementforcurativecarewhereitispossibletoprovideit(SmithandAloudat2017).
ScopeandlimitationsofthestudyThispaperfocusesontheexperiencesofexpatriatehealthprofessionalsrespondingtotheneedsofpatientswhoaredyingorlikelytodieinahumanitariancrisis.
Thisisanimportantperspective,butstillalimitedangleofview.
Investigatinghowpatients,theirfamilies,andlocalcommunitiesandhealthprofessionalsviewandexperiencethesesituationsisessentialforbetterunder-standingwhatisatstakeandforwhom.
Ourlargerresearchprojectinvolvesin-depthfieldresearchinhu-manitariansettings,includingperspectivesfrompatientsandtheirfamilies.
Theseinquirieswillprovideadditionalvantagepointsforunderstandingthistopic.
Severallimita-tionsarerelevanttotheanalysispresentedhere.
Ourpur-posivesamplingstrategywasonlypartiallysuccessful.
MostoftheparticipantswereEuropeansorNorthAmericanswhoprimarilyworkedwiththelargestoftheinternationalNGOs.
Thisdoesnotreflectthewiderangeofnationalitiesofexpatriatehumanitarianprofessionals,orthespectrumofhumanitarianorganizations,andhasundoubtedlyshapedtherangeofexperiencesandethicaloutlooksoftheparticipants.
ConclusionDeathanddyingareinescapableinhumanitariancrises.
Increasedattentionisbeingdirectedtowardquestionsrelatedtowhyitisimportantforhumanitarianorganiza-tionstorespondcompassionatelyandinajustmannertotheneedsofthesepatients,andhowtheyoughttoplanfor,implement,andassesstheseefforts.
Thestudyreportedhereprovidesimportantinsightintothemoralexperiencesofhumanitarianhealthprofessionalswhoencountersuchpatientsandhighlightssomeimportantaspectsofwhatisatstakeinthesesituations.
Theirper-spectivesspeaktoboththeessentialimportanceandcomplexitiesofcontextuallyappropriatepalliativecare.
Wehopethatitwillalsoencourageandsupportfurtherdialogueinthehumanitariansectoronthistopic.
Itiscrucialthathumanitarianhealthcareprofessionalsareprepared,supported,andresourcedinwaysthatenablethemtoattendtothesufferingandupholdthedignityofsomeoftheirmostvulnerablepatients:individualswhoaredyingorlikelytodieinhumanitariancrises.
Endnote1Atthetimeofwriting,aseconddraftoftherevisionwasavailableonline(SphereProject2017).
AbbreviationsLMICs:Low-andmedium-incomecountries;NGO:Non-governmentalorganization;WHO:WorldHealthOrganizationAcknowledgementsWearegratefultothestudyparticipantsforsharingtheirexperienceswithus,toRachelYantziforherassistancewithformattingthemanuscript,andtotheothermembersofourresearchteam,LaurieElit,LyndaRedwood-Campbell,OliveWahoush,CorinneSchuster-Wallace,ErynnMonette,MadelineMcDonald,RossUpshur,andJhalokRonjanTalukdar,fortheircontributionstoourbroaderresearchstudy.
FundingTheresearchpresentedinthisarticlewassupportedbyagrantfromElrha'sResearchforHealthinHumanitarianCrisesprogramme(Project#19775:Aidwhenthereis"nothinglefttooffer":Astudyofethicsandpalliativecareduringinternationalhumanitarianaction).
TheResearchforHealthinHumanitarianCrises(R2HC)programmeaimstoimprovehealthoutcomesbystrengtheningtheevidencebaseforpublichealthinterventionsinhumanitariancrises.
Visitwww.
elrha.
org/work/r2hcformoreinformation.
TheR2HCprogrammeisfundedequallybytheWellcomeTrustandDFID,withElrhaoverseeingtheprogramme'sexecutionandmanagement.
MatthewHuntissupportedbyaResearchScholarAwardfromtheFondsdeRechercheduQuebec-Santé,andLisaSchwartzissupportedbytheArnoldLJohnsonChairinHealthCareEthics.
Authors'contributionsMH,AC,andKBdevelopedtheinitialideaforthismanuscript.
MHwrotethefirstdraft,andallauthorsmadesubstantialcontributionsasthepaperwasrevised.
SdLandENconductedinterviewswithparticipants.
GKandACconductedinitialcodingofinterviewtranscripts.
Allauthorsreadtheinterviewtranscriptsandparticipatedinthedataanalysis.
Allauthorsapprovedthefinalversionofthemanuscript.
Author'sinformationMatthewHuntisanassociateprofessorattheSchoolofPhysicalandOccupationalTherapyofMcGillUniversityandanassociatememberoftheBiomedicalEthicsUnit.
Heconductsethicsresearchintheareasofglobalhealthandrehabilitationandco-leadstheHumanitarianHealthEthicsRe-searchGroup(humanitarianhealthethics.
net).
AniChénierisananthropologistwhoseworkexploresthewaysmortuaryandcommemorativematerialcultureenactandtransformsocialimaginaries.
SheisaresearchcoordinatorwiththeHumanitarianHealthEthicsResearchGroupatMcMasterUniversity.
KevinBezansonisapalliativecareconsultantfortheNorthwesternOntarioregionandbasedinThunderBay,Ontario,Canada,withclinical,research,andprogramdevelopmentexperiencemainlyinMalawiandEthiopia.
ElyséeNouvetisamedicalanthropologistandanAssistantProfessorintheSchoolofHealthStudies(GlobalHealth)atWesternUniversityinLondon,Ontario.
Herworkfocusesonlivedexperiencesoftrans-nationalaidandcare.
Sheisaco-leadoftheHumanitarianHealthEthicsResearchGroup.
CarrieBernardisafamilyphysicianandpalliativeleadfortheQueenSquareFamilyHealthTeaminBrampton,Ontario.
SheistheAssociateProgramDirectorofthePostgraduateFamilyMedicineprogramattheUniversityofTorontoandamemberoftheHumanitarianHealthEthicsResearchGroup.
SonyadeLaatisascholarofhistoriesofhumanitarianphotography.
CurrentprojectsincludephotographsofrefugeesfromtheFirstWorldWar,thevisualarchivesoftheCanadianInternationalDevelopmentAgency,andprojectsonphoto-basedoralhistoriesofhumanitarianaction.
GauthamKrishnarajisaresearchassistantwiththeHumanitarianHealthEthicsResearchGroupatMcMasterUniversity.
HeiscurrentlydeployedasanAgaHuntetal.
JournalofInternationalHumanitarianAction(2018)3:12Page12of13KhanFoundationCanadaInternationalYouthFellow,supportingthehealthandeducationinitiativesoftheMadrasaEarlyChildhoodProgram—Kenya.
LisaSchwartzisaprofessorintheDepartmentofHealthResearchMethodsandImpact(HEI)atMcMasterUniversityandanassociatememberoftheDepartmentofPhilosophy.
SheistheArnoldLJohnsonChairinHealthCareEthicsandisaco-leadoftheHumanitarianHealthEthicsResearchGroup.
LisaisalsoamemberoftheMédecinsSansFrontièresEthicsReviewBoard.
CompetinginterestsTheauthorsdeclarethattheyhavenocompetinginterests.
Publisher'sNoteSpringerNatureremainsneutralwithregardtojurisdictionalclaimsinpublishedmapsandinstitutionalaffiliations.
Authordetails1SchoolofPhysicalandOccupationalTherapy,McGillUniversity,845SherbrookeStreetWest,Montreal,Quebec,Canada.
2CentreforInterdisciplinaryResearchonRehabilitation,Montreal,Quebec,Canada.
3HumanitarianHealthEthicsResearchGroup,McMasterUniversity,1280MainStreetWest,Hamilton,Ontario,Canada.
4NorthernOntarioSchoolofMedicine,LakeheadandLaurentianUniversities,ThunderBayRegionalHealthSciencesCentre,980OliverRoad,ThunderBay,Ontario,Canada.
5SchoolofHealthStudies,WesternUniversity,1151RichmondStreet,London,Ontario,Canada.
6DepartmentofCommunityandFamilyMedicine,UniversityofToronto,Toronto,Canada.
7DepartmentofFamilyMedicine,McMasterUniversity,Hamilton,Canada.
8DepartmentofHealthResearchMethods&Impact,McMasterUniversity,1280MainStreetWest,Hamilton,Ontario,Canada.
Received:10April2018Accepted:27June2018ReferencesBarclayL(2018)Dignitarianmedicalethics.
JMedEthics44(1):62–67.
https://doi.
org/10.
1136/medethics-2017-104467BehrensKG(2013)TowardsanindigenousAfricanbioethics.
SAfrJBioethLaw6(1):32–35DeLimaL,KrakauerEL,LorenzK,PraillD,MacDonaldN,DoyleD(2007)Ensuringpalliativemedicineavailability:thedevelopmentoftheIAHPClistofessentialmedicinesforpalliativecare.
JPainSymptomManag33(5):521–526DeWaalA(2010)Thehumanitarians'tragedy:escapableandinescapablecruelties.
Disasters34(s2):s130–s137.
https://doi.
org/10.
1111/j.
1467-7717.
2010.
01149.
xElrha(2017)Takepartinthepalliativecareinhumanitarianactionsurveynow.
http://www.
elrha.
org/news/take-part-palliative-care-humanitarian-action-survey-now/.
Accessed13Mar2018GaudioFD,HichenbergS,EisenbergM,KerrE,ZaiderTI,KissaneDW(2013)Latinovaluesinthecontextofpalliativecare:illustrativecasesfromthefamilyfocusedgrieftherapytrial.
AmJHospPalliatCare30(3):271–278GiannouC,BaldanM(2009)Warsurgery:workingwithlimitedresourcesinarmedconflictandothersituationsofviolence,vol1Availableviahttps://www.
icrc.
org/en/publication/0973-war-surgery-working-limited-resources-armed-conflict-and-other-situations-violence.
Accessed20June2018GyselsM,PellC,StrausL,PoolR(2011)Endoflifecareinsub-SaharanAfrica:asystematicreviewofthequalitativeliterature.
BMCPalliatCare10(1):6HajjarRR,CharalambousHA,BaiderL,SilbermannM(2015)Internationalpalliativecare:MiddleEastexperienceasamodelforglobalpalliativecare.
ClinGeriatrMed31(2):281–294HorningJ,SchwartzL,HuntM,Williams-JonesB(2017)"Ifyouletitgettoyou…":moraldistress,ego-depletion,andmentalhealthamongmilitaryhealthcareprovidersindeployedservice.
In:MesselkenD,WinklerD(eds)Ethicalchallengesformilitaryhealthcarepersonnel:dealingwithepidemics.
Routledge,London,pp71–91HumanitarianHealthEthicsResearchGroup(2018)Palliativecareinhumanitarianresponse.
https://humanitarianhealthethics.
net/home/research/hhe-research-studies/pall-iphc/.
Accessed13Mar2018HuntM,BezansonK,BernardC(2017)Makingspaceforpalliativecareinhumanitarianaction:Reflectionsonobstaclestotheintegrationofpalliativecareapproachesinhumanitarianhealthcare.
Elrha.
http://www.
elrha.
org/r2hc-blog/making-space-palliative-care-humanitarian-action-reflections-obstacles-integration-palliative-care-approaches-humanitarian-healthcare.
Accessed13Mar2018HuntMR,CarnevaleFA(2011)Moralexperience:aframeworkforbioethicsresearch.
JMedEthics37(11):658–662InternationalChildren'sPalliativeCareNetwork(2008)TheICPCNcharterofrightsforlifelimitedandlifethreatenedchildrenhttp://www.
icpcn.
org/icpcn-charter/.
Accessed22Mar2018JametonA(1993)Dilemmasofmoraldistress:moralresponsibilityandnursingpractice.
AWHONNSClinIssuesPerinatWomensHealthNurs4(4):542–551KleinmanA(1999)Moralexperienceandethicalreflection:canethnographyreconcilethemAquandaryfor"thenewbioethics".
Daedalus128(4):69–97KnaulFM,FarmerPE,KrakaeurEL,DeLimaL,BhadeliaA,JiangKweteX,Arreola-OrnelasH,Gómez-DantésO,RodriguezNM,AlleyneGAO,ConnorSR,HunterDJ,LohmanD,RadbruchL,delRocíoSáenzMadrigalM,AtunR,FoleyKM,FrenkJ,JamisonDT,RajagopalMR,onbehalfoftheLancetCommissiononPalliativeCareandPainReliefStudyGroup(2018)Alleviatingtheaccessabyssinpalliativecareandpainrelief—animperativeofuniversalhealthcoverage:theLancetCommissionreport.
Lancet391(10128):1391–1454LamontagneF,FowlerRA,AdhikariNK,MurthyS,Brett-MajorDM,JacobsMetal(2018)Evidence-basedguidelinesforsupportivecareofpatientswithEbolavirusdisease.
Lancet391(10121):700–708LeporaC,GoodinRE(2013)Oncomplicityandcompromise.
OxfordUniversityPress,OxfordLincolnYS,LynhamSA,GubaEG(2011)Paradigmaticcontroversies,contradictions,andemergingconfluences,revisited.
In:DenzinNK,LincolnYS(eds)TheSagehandbookofqualitativeresearch,4thedn.
Sage,LosAngeles,pp97–128MacklinR(2003)Dignityisauselessconcept.
BMJ237:1419.
https://doi.
org/10.
1136/bmj.
327.
7429.
1419MarstonJ,DeLimaL,PowellRA(2015)Palliativecareincomplexhumanitariancrisisresponses.
Lancet386(10007):1940MédecinsDuMonde(2016)Soinspalliatifspédiatriques:Quandguérirn'estpluspossible,toutn'estpasterminé.
https://medecinsdumonde.
ch/activites/spp/le-projet/.
Accessed13Mar2018NickersonJW,AttaranA(2012)Theinadequatetreatmentofpain:collateraldamagefromthewarondrugs.
PLoSMed9(1):e1001153NouvetE,SivaramM,BezansonK,KrishnarajG,HuntM,deLaatS,SangerS,BanfieldL,EscobioRodriguezPF,SchwartzLJ(2018)Palliativecareinhumanitariancrises:areviewoftheliterature.
IntJHumanitarianAction3(5).
doi:https://doi.
org/10.
1186/s41018-018-0033-8PowellRA,SchwartzL,NouvetEetal(2017)Palliativecareinhumanitariancrises:alwayssomethingtooffer.
Lancet389:1498–1499.
https://doi.
org/10.
1016/S0140-6736(17)30978-9SchneiderM,PautexS,ChappuisF(2017)WhatdohumanitarianemergencyorganizationsdoaboutpalliativecareAsystematicreview.
MedConflSurviv33(4):263–272.
https://doi.
org/10.
1080/13623699.
2017.
1409167SmithJ,AloudatT(2017)Palliativecareinhumanitarianmedicine.
PalliatMed31:99–101.
https://doi.
org/10.
1177/0269216316686258SphereProject(2011a)Glossary:humanitarianaction.
http://www.
sphereproject.
org/handbook/glossary/l=H.
Accessed13Mar2018SphereProject(2011b)Humanitariancharter.
http://www.
spherehandbook.
org/en/the-humanitarian-charter/.
Accessed13Mar2018SphereProject(2017)Draft2oftheSphereHandbooknowreadyforreviewandfeedback.
http://www.
sphereproject.
org/handbook/revision-sphere-handbook/draft-ready-for-feedback/.
Accessed19Mar2018TerryF(2002)CondemnedtorepeatTheparadoxofhumanitarianaction.
CornellUniversityPress,IthacaThorneS(2016)Interpretivedescription:qualitativeresearchforappliedpractice,vol2.
Routledge,NewYorkThorneS,KirkhamSR,O'Flynn-MageeK(2004)Theanalyticchallengeininterpretivedescription.
IntJQualMethods3(1):1–11WebsterGC,BaylisFE(2000)Moralresidue.
In:RubinSB,ZolothL(eds)Marginoferror:theethicsofmistakesinthepracticeofmedicine.
UniversityPublishingGroup,Hagerstown,pp217–230WHO(2018)WHOmediacentrefactsheetonpalliativecare.
WorldHealthOrganization.
http://www.
who.
int/mediacentre/factsheets/fs402/en/.
Accessed20June2018Huntetal.
JournalofInternationalHumanitarianAction(2018)3:12Page13of13
Internationalnon-governmentalorganizationsrespondtomanyofthesecrisesandprovidehealthcareinsettingsrangingfromafieldhospitaldeployedafteranearthquake,toahealthclinicinalongstandingrefugeecamp,toatreatmentcenterduringaninfectiousdiseaseoutbreak.
Theprimaryfocusoftheseactivitiesistosavelives.
However,inevitably,manypatientscannotbesaved.
Weundertookaninterpretivedescriptionstudytoinvestigatehumanitarianpolicy-makerandcareproviders'experiencesandperceptionsofpalliativecareduringhumanitariancrises.
Inthispaper,wereportoninterviewswith23healthprofessionals,11ofwhomalsohadexperienceaspolicy-makerswithinahumanitarianorganization.
Weusetheconceptofmoralexperienceasananalyticlens:participants'experiencesofvaluesthattheyheldtobeimportantbeingrealizedorthwartedastheyrespondedtotheneedsofpatientswhoweredyingorlikelytodie.
Weidentifiedfivethemesrelatedtoparticipants'moralexperiences,allofwhichrelatetovaluesofcompassionintheprovisionofcare,andjusticeinaccessingit.
(1)Participantsdescribedinterveningtoeasethesufferingofdyingpatientsasaninherentaspectofhumanitarianismandtheirdutyashealthprofessionals.
(2)Participantsalsoexpressedthatupholdingdignitywasofcriticalimportance,stemmingfromarecognitionofsharedhumanityandasanactofrespect.
(3)Sincehumanitarianactionisprovidedinsituationsofscarcity,prioritizationisinescapable.
Acknowledgingtheprimacyofcurativecareinemergencies,participantsalsoemphasizedtheimportanceofensuringthatcareforthedyingwasattendedto,includingduringtriage.
(4)Participantsreportedworkingwithinandpushingagainstsystemicconstraintssuchaslegalorlogisticalbarrierstoopioids,lackofguidelines,andconflictingviewswithcolleagues.
(5)Giventhestakesinvolved,participantsfeltaheavyweightofresponsibilityanddescribedtheirchallengesincarryingit.
Thesefindingsilluminateexperiencesrespondingtopatientswhoaredyingorlikelytodie,andhowtheseconnectwiththevaluesofhumanitarianhealthprofessionals,sometimesresultingindissonancebetweenvaluesandactions.
Theyalsopointtotheneedtomakemorespaceforpalliative,alongsidecurative,approachestocareinsituationsofhumanitariancrises,ideallybyfurtherintegratingthem.
Keywords:Disaster,End-of-life,Epidemic,Ethics,Humanitariancrisis,Moralexperience,Non-governmentalorganizations,Palliativecare,Reliefwork,Values,War*Correspondence:matthew.
hunt@mcgill.
ca1SchoolofPhysicalandOccupationalTherapy,McGillUniversity,845SherbrookeStreetWest,Montreal,Quebec,Canada2CentreforInterdisciplinaryResearchonRehabilitation,Montreal,Quebec,CanadaFulllistofauthorinformationisavailableattheendofthearticleJournalofInternationalHumanitarianActionTheAuthor(s).
2018OpenAccessThisarticleisdistributedunderthetermsoftheCreativeCommonsAttribution4.
0InternationalLicense(http://creativecommons.
org/licenses/by/4.
0/),whichpermitsunrestricteduse,distribution,andreproductioninanymedium,providedyougiveappropriatecredittotheoriginalauthor(s)andthesource,providealinktotheCreativeCommonslicense,andindicateifchangesweremade.
Huntetal.
JournalofInternationalHumanitarianAction(2018)3:12https://doi.
org/10.
1186/s41018-018-0040-9IntroductionHumanitarianhealthcareaimstosaveandsafeguardthelivesofpeoplecaughtupinsituationsofcrisis.
Thisisenactedindiversesettings:internationalnon-governmentalorganizations(NGOs)implementvaccinationandfeedingprograms,setuptreatmentcentersduringoutbreaksofinfectiousdiseasessuchascholeraandEbola,providepri-marycareinrefugeecamps,andestablishfieldhospitalstodeliversurgicalcareduringwarsandfollowingnaturaldisasters,amongstmanyotheractions.
Despitethebestintentionsanddedicatedcareofhumanitarians,manypa-tientswilldieduetoinjuryorincurabledisease.
Thisisaninescapablereality,especiallygiventheprecarityandresourcescarcitythatcharacterizehumanitariancrises.
Theoverridingimperativeofsavinglivesinhumanitar-ianhealthcare,however,hasoftenleftlimitedroomforaddressingsufferinganddignity,especiallyforindivid-ualswhoaredying,inhumanitariansettings(Powelletal.
2017).
Therehasalsobeenalackofguidanceandsupportrelatedtocaringfordyingpatientsduringhu-manitariancrisis(Nouvetetal.
2018),asituationwhichmayincreaseuncertaintyandleadtomoraldistress.
Inthepastfewyears,increasedattentionhasbeendi-rectedtowardpalliativecareprovisionbyhumanitarianhealthprofessionals.
TheWorldHealthOrganization(WHO)definespalliativecareas"anapproachthatim-provesthequalityoflifeofpatients(adultsandchildren)andtheirfamilieswhoarefacingproblemsassociatedwithlife-threateningillness.
Itpreventsandrelievessuf-feringthroughtheearlyidentification,correctassess-mentandtreatmentofpainandotherproblems,whetherphysical,psychosocialorspiritual"(WHO2018).
Commentatorshavearguedfortheimportanceofpalliativecareprovisioninsituationsofwar,disaster,andepidemic(Marstonetal.
2015;SmithandAloudat2017),withPowelletal.
arguingthatitshouldbecon-sidered"anintegralcomponentofreliefstrategies"(2017:1498).
SomeNGOshaveestablishedpoliciestosupporttheirfieldteamsinprovidingcareforpatientswhoarenotexpectedtosurvive,suchastheInter-nationalCommitteeoftheRedCross'striageguidelineswhichidentifyminimumcarestandardsforthesepa-tients(GiannouandBaldan2009).
Broadereffortsthatcrossthehumanitarianfieldarealsounderway,includ-inganinitiativetointroduceanewchapterintheSphereHandbook:HumanitarianCharterandMinimumStan-dardsinHumanitarianResponseaddressing"reliefofsufferingandend-of-lifecare.
"1Evidence-basedstan-dardsforsupportivecareinEbolaTreatmentCentershavealsobeendevelopedandincluderecommendationsforpaincontrolandaddressingpsychologicaldistress(Lamontagneetal.
2018).
Theseinitiativeshavethepotentialtofurtherfore-groundtheneedforpalliativecareinhumanitariansettingsandestablishguidancetohelporientpractice.
Thereremains,however,littleinformationaboutpalliativecareinterventionscarriedoutaspartofthehumanitarianresponsetocrises(Schneideretal.
2017),includingexpe-riencesofpatients,families,andcareproviders.
Withthegoalofbetterunderstandingopportunities,obstacles,andexperiencesofpalliativecareprovisioninhumanitariancrises,wehaveundertakenamulti-stageresearchprojectthatincludesasurvey,interviewswithhumanitarianhealthprofessionalsandpolicy-makers,andin-depthcasestudies,includinginterviewswithpatients,families,andhealthprofessionalsinRwanda,Jordan,andGuinée(HumanitarianHealthEthicsResearchGroup2018).
Inthispaper,wefocusonexperiencesofprovidersofcareandreportoninterviewsweconductedwith23healthprofes-sionals,11ofwhomalsohadexperienceaspolicy-makerswithinhumanitarianNGOs.
Ouranalysisfocusesontheirmoralexperiences,thatissituationsinwhichtheyexpe-riencedvaluestheyheldtobeimportantasbeingrealizedorthwarted(HuntandCarnevale2011)astheyrespondedtotheneedsofpatientswhoweredyingorlikelytodieinahumanitariancrisis.
MethodsThisinquirywasguidedbyinterpretivedescriptionmeth-odology(Thorne2016)andwasundertakenwithinacon-structivistparadigminwhichhumanexperienceisunderstoodassubjective,local,sociallyandexperientiallybased,andculturallyandhistoricallyspecific(Lincolnetal.
2011).
Interpretivedescriptionaimstodevelopa"coherentconceptualdescriptionthattapsthematicpatternsandcommonalitiesbelievedtocharacterizethephenomenonthatisbeingstudiedandalsoac-countsfortheinevitableindividualvariationswithinthem"(Thorneetal.
2004:7).
Here,wereportonouranalysisoftheinterviewsan-sweringthefollowingquestion:"Whatarethemoralexpe-riencesofhumanitarianhealthprofessionalsastheyrespondtotheneedsofindividualswhoaredyingorlikelytodieduringahumanitariancrisis"Thisanalysisisguidedbythefollowingunderstandingofmoralexperi-ence:"Moralexperienceencompassesaperson'ssensethatvaluesthatheorshedeemsimportantarebeingreal-izedorthwartedineverydaylife.
Thisincludesaperson'sinterpretationsofalivedencounter,orasetofliveden-counters,thatfallonspectrumsofright-wrong,good-bad,orjust-unjust"(HuntandCarnevale2011:659).
Thus,inquiryintomoralexperienceaimstoilluminate"thelocalprocesses(collective,interpersonal,subjective)thatrealize(enact)valuesinordinaryliving"(Kleinman1999:71).
EthicsThisstudywasreviewedandapprovedbytheHamiltonIntegratedResearchEthicsBoardatMcMasterUniversity,Huntetal.
JournalofInternationalHumanitarianAction(2018)3:12Page2of13andtheMcGillFacultyofMedicine'sInstitutionalReviewBoard.
Allparticipantsprovidedwritteninformedconsenttoparticipateinthestudy.
RecruitmentWerecruitedparticipantsusingfourapproaches.
First,wedistributedinformationaboutthestudyonsocialmedia(viaourresearchgroup'sTwitterandFacebookaccounts).
Second,wesharedinformationwithinourprofessionalnetworkswhichresultedintherecruitmentof11participants.
Third,attheendofthesurveythatwasconductedbyourresearchteamaspartofthebroaderproject(seeElrha2017),weinvitedsurveyre-spondentstoindicatetheirinterestinalsoparticipatinginaninterview.
Nineparticipantswererecruitedthroughthesurvey.
Finally,werecruitedthreepartici-pantsusingsnowballsampling,askingintervieweestosuggestotherswhomightbeinterestedandeligibletoparticipateinthestudy.
Throughoutthisprocess,weattemptedtorecruitadiversegroupofparticipants,in-cludingmenandwomen,andindividualsaffiliatedwithdifferentorganizations,comingfromdifferentregionsoftheworld,andwithexperienceworkingindifferenthu-manitariansettingsandindifferentcapacities.
ParticipantsThispaperreportsontheanalysisofinterviewswith23healthprofessionals(16physicians,6nurses,andonephysicaltherapist),11ofwhomhadalsoworkedaspolicy-makerswithahumanitarianorganization.
Inthiscomponentofthestudy,wehadalsointerviewedanon-clinicianpolicy-makerbutthatinterviewisnotin-cludedintheanalysispresentedhereduetoourfocusonexperiencesofcareprovision.
The23participantswereaffiliatedwith18differentorganizationsandin-cluded11menand12women.
MostoftheparticipantshadworkedwithlargerinternationalorganizationsbasedinEuropeorNorthAmerica.
Ourpurposivesamplingwaslimitedinthatparticipantsincludedmorephysi-cians(16)thanotherhealthprofessionals(7)andmoreindividualsfromhigh-(19)thanlow-ormiddle-incomecountries(LMICs)(4).
InterviewsInterviewswereconductedbetweenNovember2016andMay2017,inEnglishorFrenchaccordingtotheprefer-enceoftheparticipant,andfollowedaninterviewguide.
Wecreatedtwoversionsoftheinterviewguide(oneforparticipantswhohadexperienceonlyasclinicians,andoneforparticipantswhoalsohadexperienceasapolicy-maker),andeachwasrefinedbasedonfeedbackfromexperiencedhumanitarianhealthprofessionalsandpolicy-makers,andpersonswithexpertiseinpalliativecare.
AllinterviewswereconductedbySkypeortelephoneduetothegeographicdispersionofthepartic-ipants.
Interviewsrangedfrom49to92mininduration(average65min).
AnalysisWeinitiatedtheanalysisoftheinterviewsastranscriptsbecameavailable.
InductivecodingwasdonebytwoteammembersandorganizedusingNVivosoftware.
Therewereseparatecodersforthepolicy-maker(GK)andhealthprofessional(AC)interviews.
Ateammember(MH)independentlycodedsectionsoffourtranscripts(twoforpolicy-makersandtwoforhealthprofessionals),andthreeteammembers(KB,CBandEN)independentlycodedonepolicy-makerinterview.
Theprovisionalcodebookwasrefinedthroughdiscussionwiththewholeteamandthroughcomparisonofcodedtranscripts.
Ananalyticstructurerelatedtomoralexperiencewasthendevelopedbythreeteammembers(MH,KB,andAC)byrepeatedandclosereadingofthetranscripts,useofvisualmatricesandconceptmaps,anddiscussion.
Onceaninitialanalyticstructurewasestablished,ateammember(MH)rereadalltranscriptsinlightofthisemerginganalysistotestitsconsistencyandcomprehensiveness.
Theanalyticstruc-turewasthenrevisedthroughteamdiscussion.
ResultsParticipantsdescribedanddiscussedexperiencesofpal-liativecareprovisionandreflectedonitsplaceinhu-manitarianresponse.
Usingthelensofmoralexperience,weanalyzednarrativesofcareinwhichparticipantsexperiencedvaluestheyheldtobeimportantasbeingrealizedorthwarted.
Manyvalueswereimplicatedinthesedescriptions.
Theyclusteredaroundtwounder-lyingcommitments:tojusticeinaccesstocareandcom-passioninprovisionofcare.
Throughaprocessofinductiveanalysis,weidentifiedfiveinterlinkingdimen-sionsofmoralexperienceinrelationtocaringforpa-tientswhoweredyingorlikelytodie:actingtoeasesuffering,upholdingdignity,balancingcarepriorities,workingwithinandresistingsystemicconstraints,andbearingtheweightofresponsibility.
Tworelatetowhatmanyunderstoodasimperatives:actingtoeasesuffer-ing,andupholdingandpreservingdignity.
Theotherthreerelatetoparticipants'experienceofworkingtomeettheseimperativesintheheavilyconstrainedcon-textofhumanitarianaction:balancingcarepriorities,workingwithinandresistingsystemicconstraints,andbearingtheweightofresponsibility.
Distinctyetcon-nectedintheunderlyingcommitmentstojusticeandcompassionthatinspiresandinformsthem,thesethemesshedlightonwhyandhowhealthprofessionalsengagedinhumanitariancrisesexperiencetheneedsforpalliativecareprovisionasmorallyimportant,some-timeshaunting,experiences.
Huntetal.
JournalofInternationalHumanitarianAction(2018)3:12Page3of13ActingtoeasesufferingOurparticipantsviewedactingtoeasesufferingasanintegralcomponentofgoodcareforallpatientsinhumanitariansettings,butespeciallyimportantforindivid-ualswhoaredyingorlikelytodie.
Theyalsodescribedhow,duetovariousfeaturesofwars,disasters,orepi-demics,thisdimensionofcaremaybeneglectedoreclipsedbyanoverwhelmingconcernforsavinglivesandstewardinglimitedresources.
Asaresult,andillustratedinmanyofthenarrativesrecountedbyparticipants,sufferingistooofteninsufficientlyaddressed,evenmoresoforpeoplewhoaredying.
Nonetheless,whencurativecarewasunavailableorinappropriate,participantsarguedthatpal-liativecareshouldbeprovidedandthataddressingsymp-tomsandrelievingpainwasanobligationofhumanitarianhealthprofessionals,andthatnotdoingsorepresentedaninjustice.
Aphysicianinvolvedindevelopinghumanitarianpalliativecareguidelinesarguedstronglyfortheimport-anceofalleviatingsuffering,since"notgivingpalliativecareandpaintreatmentisexactlylikenon-assistancetopersonsindangerorlikeacceptingtorture.
Becausesomepainsareliketorture"(P1).
Whilemakingtheseassertionsabouttheimportanceofalleviatingsuffering,participantsconsist-entlyexpressedthatlifesavingwastheprimaryfocusofhumanitarianhealthcare.
Generally,theyviewedalleviationofsuffering,includingfordyingpatients,assomethingthatwascompatiblewithandcomplementarytothisfocus.
Severallinkedthisclaimtothemandateofhumanitar-ianaction,since"ahumanitarianorganization…[has]avocationofcaringforthemostfragilepeopleintheworld"(P4).
Giventheextremevulnerabilityofindivid-ualswhoaredying,addressingtheirsufferingwasde-scribedasinherenttothevisionofhumanitarianaction.
Aphysicianinvolvedintrainingandpolicy-makingataninternationalNGOtookahistoricalperspective,statingthatpalliationwaspartofthe"DNA"(P10)ofhumani-tarianismasitwascentraltothefoundingoftheRedCrossmovementthroughtheactionsofHenriDunantattheBattleofSolferinoin1859.
Thisalignswiththeideasexpressedbyparticipantswhoemphasizedthateffortstoalleviatesufferingwereconsistentwith,andevenamountedtoareclaimingof,humanitarianvalues.
Inthissense,theseparticipantsfeltthathumanitariansfallshortoftheiridealsand"missthemark"(P17)iftheydonotaddresssuffering,especiallyofdyingpatients.
Anursewhohadtakenpartinthehumanitarianre-sponseafteranearthquakeandduringacivilwardescribedseveralsituationswhereshesoughttoaddresspatients'suffering,aswellascircumstanceswhendoingsowasespeciallydifficult.
Inherinterview,shefre-quentlyreturnedtoasituationwhereactivefightinginCentralAfricaledtoherteambeing"inundatedwithhundredsofpatients"(P19).
Sheassertedthatevenincircumstanceswhentriagingpatientswasunavoidable:…ifyoudon'tprovidesomethingforpain,andyoudon'tdothelittlethingsthen–thenyou'relosingalittlebitofwhyyou'reeventhereandthewholemoralpiecetoit…thehumanitarianpiece.
Otherwiseyou'rejustabunchofmedicsrunningaroundinthefield,tryingto…stopthebleeding,butwhen–ifyou'regonnabehumanitarians,thenyouhavetoreallylookatthathumanpiece…(P19)Highlightedactionstoalleviatesufferingincludednotonlyprovidinganalgesicsbutalsoprovidingwater,put-tingupasunshade,andhavingsomeonestaywithgrievouslyinjuredpatientswhoweretriagedtonotre-ceivelifesavingcare.
Failuretoengageinsuchacts,shefelt,wouldrepresenthumanitariansfailingtoliveuptotheirvalues.
Alongwithmasscasualtytriagesituations,careprovisionindiseaseoutbreakswasalsodiscussedbymanypartici-pantsasacontextwhereattentiontosufferingwasex-tremelychallenging,yetnecessary.
Whileafewstorieswererelatedtooutbreaksofcholeraorotherdiseases,mostweretoldaboutthe2014–15Ebolavirusdiseaseout-breakinWestAfricatowhichsevenoftheparticipantshadresponded.
Inthissetting,curativeoptionswerenotavailable.
Anursereported,"whenIstartedwehadlikea70%mortalityrate,sobasicallyallweweredoingwaspalliativecare,Imeanwewerejustmakingpeoplecom-fortable…attheendoftheirlives"(P11).
SeveralparticipantsdescribedsituationsinwhichEbolapatientsweredyingbutinfectioncontrolmeasuresimpededthealleviationofsuffering.
Theseconcernswereparticularlyacutewhenpatientswerebleedingandvomitingorhaddiarrhea.
AphysiciandescribedcominguponanEbolapatientwhowasimminentlydyingbutwhohadpulledoutherIVandtheneedlecouldnotbefound.
WhileencumberedbytheirPersonalProtectiveEquipment,shedescribedenteringtheroomwithacolleagueand:keepingsortofmybuddysafe…andfindingthesharp,that's,that'skindofwhathedidfirst,youknow,findingthehangingneedle…Ishouldhavetriedtoatleastmakehercomfortablewhileweweredoingthat,andI'mtryingtothinkofthetime,howmuchtimepassedbetweenusseeingherandherdyingand…itwaslike20minutes…soIthinkeven…duringthat20minuteswecould'vedonesomething.
Icouldhavethoughttodomoreorjustplannedbetter.
(P3)Sheexpressedregretthatshehadneitherattendedtothepatient'sdistressnorbeensufficientlyattentivetoherinthemomentofherdeath.
AphysicianwhohadcometoWestAfricafromanotherAfricancountrytoparticipateintheEbolaresponseHuntetal.
JournalofInternationalHumanitarianAction(2018)3:12Page4of13describedasituationwhenhefeltthatpalliativecarehadbeendoneespeciallywell:Yes,therewasthisboy,…[he]presentedtothe[EbolaTreatmentCenter],hehaddiarrheaandvomiting,and…whatwedidaspalliation,becausehediedeventually,wasIVfluids.
Irememberthatfluidsverywell,buthekeptstoolingandvomiting,andattimeswehadtogoinoneortwotimes,andusuallywegoinshifts,themorningshift,theafternoonandthenightshift,soatonepointweweregoinginmorefrequentlybecauseofhim.
Wedidalotoffluidresuscitation.
Hehadalotofabdominalpain,alotofabdominalpain,sowetriedtousealotofpainkillers.
Morphine,Tramadol,triedtouseallthat.
WhatelsedidwedoIthinkpsychosocialsupport…Andwhenwethinkthepatientswouldhavegivenuponlifeandthinkeverythingissobad,wewouldtrytosendthePsychosocialTeamtogotalktothem…AndIthink[that]particulardayhesortofdeteriorated,andbytheendofthedaywelosthim.
Therewereotherinstances,butthatwastheincidentthatittookmealongtimetotrytoforgetit.
(P5)Participantsalsospokeabouttheimportanceoffamily.
Manyrecognizedthatduringacrisis(anearthquakeoranepidemic,forexample)patientsthemselvesmayhavelostfamilymembersandbemourningtheirownlosses,andthatthelossoffamilymembersmaycompoundthefeelingofisolationduringtheirowndyingprocess.
ThiswasparticularlysoduringtheEbolaepidemicwhensomepatientshave"alreadylostyouknow10,15peopleintheirfamilies.
Everybodyhaslostsomebody"(P11).
Enablingpatientstoremainconnectedwithfamilywaspresentedasameanstoalleviatepsychologicaldistress.
Doingsowasdescribedasespeciallyvitalandchallen-ginginEbolaTreatmentCenters.
Suchactionsincludedbringingpatientstotheperimeterfencetointeractwithfamilymembers,orsupportingpatientsinisolationroomstocommunicatewithfamilyusingcellphonesortablets,orbyrecordingvideomessages(P20).
Eveninamasscasualtyemergency,aparticipantsuggestedtheimportanceofcreatingopportunitiesforrelativestobetogether(P14).
Attentiontosufferingwascloselyrelatedtoconcernforupholdingthedignityofdyingpatients,andthetwogoalswereoftendiscussedbyparticipantsasinter-twined.
Forexample,whenreplyingintheaffirmativethatprovidingpalliativecareshouldbeanobligationofhumanitarianorganizationsinemergencysituations,aphysicianlinkedsuffering,preservinghumanidentity,anddignifieddeath:"ifanybodyisdying,theyshoulddieasahumanandnotbelefttosuffer"and"Wherethere'sanemergencyandanybodydies,youshoulddieindignity"(P5).
Inthefollowingsection,weforegroundhowparticipantsdiscussedeffortstoupholdandpre-servehumandignity.
UpholdingdignityParticipantsconsistentlyemphasizedtheneedforhu-manitarianhealthprofessionalstoupholdthedignityofdyingpatients.
Theimportanceofdoingsowasde-scribedasstemmingfromarecognitionof,andresponseto,dyingindividuals'humanityandasanactofrespectandcompassion.
Inthislight,aphysicianexpressedthathumanitarianhealthcarerequired"strongpeoplewithstrongethics,butalsowithstrongcommitmenttovalueandtorespectthedignityofpeopleandothers"(P10).
Anotherphysicianexpressedthat"evenifapatientdoesnothavecurativesolutions",heorshe"isstillahumanbeing"andrequires"decentcarefordying"(P14).
Participantsdescribedmanyactionsasdignitypromot-ing,oneinparticularbeinghumantouch.
AphysicianreportedworkinginanEbolaTreatmentCenterwheretheteamplaceda"hugefocusonsortofattemptingtofocusondignity"includingensuringyoucan"safelytouchapersonandholdapersonandcleanaperson,youknow,whentheysoilthemselvesandsoforth"(P3).
Sheexpressedthatinanepidemic,itwascriticaltoseepatientsashumanbeings,notjustaspotentialtransmit-tersofdisease.
Anotherparticipant,anurse,describedthatevenwith50patientswhostillneededtobeseenbyherteam,itwasimportanttodemonstratecompassionand"holdachild,ortositandholdsomeone'shandorstroketheirback"(P21).
Suchactionsofhumanconnec-tionwerefrequentlyemphasizedbyparticipantsastheydiscussedtheimportanceofdignityfordyingpatients.
Akeyaspectofrespectingthehumanityofdyingpa-tients—andupholdingtheirdignity—wasensuringthattheydidnotfeelabandoned.
Referringtoadyingpatientwhomshehadwitnessedbeingplacedbehindashedbe-causetheclinicwasovercrowded,anurseasked,"whatisthehumanthingtodoPutting[dyingindividuals]behindtheshedandforgettingaboutthemisnottheanswer"(P19).
Leavingafellowhumanwithoutanycareandalonewhiletheyweredyingwasframedasbothaninjusticeandanindignity:AndIthinkalsoitprovidesthepatientwiththesenseofbeingcaredforuntiltheend.
Thatyouaren't…a'lostcause,'orthatyou'vebeen…'abandoned.
'Butthatyourlifestillmatterstotheveryend,however[much]timeyoudohave,andtolivewithasmuchcomfortaspossibleuntilthattime.
(P6)Aphysicianexpresseddismaythatinacrisis,dyingpa-tientswereputtothesideanddidnotreceiveattentionand"werealreadyconsidereddeadbeforetheyevenHuntetal.
JournalofInternationalHumanitarianAction(2018)3:12Page5of13died"(P23).
Incontrast,severalparticipantsdescribedtheimportanceofusing"presencewell"(P21)andenact-ing"accompaniment"(P4)fordyingpatients.
Accom-panimentalsoextendedtosupportingpatients'families;anursedescribedprovidingsupportforthemotherofaboywhohadaseverespinalcordinjuryafterfallingoutofatreeasanactof"help[ing]hismotherwalkthroughthiswholeissue"(P19).
Thevaluethatparticipantsplacedonensuringthatdyingpatientsfeelaccompaniedandnotabandonedisfurtherillustratedbythefollowingsituation.
Aphysicianrecountedwhyshehadagreedtopraywithapatientwhenthepatientaskedhertodoso.
Thoughde-scribingherselfasnotreligious,sheexpressedthatprayingwiththepatient"basicallysaidI'mwithyou"(P18).
Narra-tivessuchasthesemakevisiblethelinkinatleastsomehumanitarianhealthcareprofessionals'mindsbetweenrespondingtopalliativecareneedswithactivepresenceandacknowledgingacommonhumanity.
Dignitywasalsoassociatedwithaddressingconcernsre-latedtoprivacy.
Forexample,anursedescribedatlengthwhyshefeltthatprovidingprivacyforadyingpatientwascrucialforherdignity:"that'sahugepieceofittoo,like–notbeingondisplayforeverybody,sohavingprivacy,Ithink,whenyou'retalkingaboutwhat'simportantinpalliativecare,thedignityaspectishuge"(P19).
Shedis-cussed,however,thatitwasimportanttoconsiderthepossibilityofimposingnormsofprivacywithoutconsult-ingthepatient.
Indeed,treatingpatientswithrespectashumanbeingswasalsolinkedtoallowingpatientstovoicepreferencesandmakechoices.
Thehumanitariancontextsometimesmakesithardforpractitionerstofollowthisideal.
Anothernurse,reflectingonherexperiencesofthe2010Haitiearthquake,notedthatwith"cross-culturalandlanguagebarriers,sometimesthepatient'sopinionsandthoughtsjustaren'tgiventhetimeandweightthattheyoughttobegiven"(P21).
Amajorityofparticipantsemphasizedtheimportanceofpreserving"culturallyvalued"(P21)and"culturallyac-ceptable"(P7)endoflifepractices,acknowledgingthatwhatconstitutesdignityandadignifieddeathisnotthesameacrosstheworld.
Thisdiversitymayraisechal-lengesforhealthprofessionals,especiallyforexpatriates,includingaphysicianwhoexpressedtheimportanceofcaring"forthosewhomaynotsurviveandwhoalsodeservea,whateveryoudefinedignifiedas,adignifieddeath"(P6).
Theculturaldimensionsofdeathanddying—includingarounddignity—ledseveralpartici-pantstosuggestthatlocalhealthprofessionalswerebestplacedtoleadpalliativecareefforts.
Theyalsosuggestedthatlocalreligiousleaderswereimportantallies,andseveralgaveexamplesofworkingcollaborativelywithsuchindividuals.
AnAfricanphysician(P5)whohadrespondedtoahumanitariancrisisinaneighboringcountrywentfurtherandsuggestedthatpalliativecareeffortsshouldbecommunity-basedwithinternationalNGOs'roleslimitedtoprovidingoversightandsupport.
Effortstoupholddignityalsoextendedbeyonddeathandincludedfamilybereavement.
Participantsdescribedtheimportanceofmemorialsandfuneralservices,in-cludingaphysicianwhoexplainedthatshechosetoat-tendamemorialserviceasawayofhonoringpatientswhohaddied(P3).
InfectioncontrolduringEbolapre-sentedmanychallengesinthisregard.
Forexample,anursereportedthatwhiletraditionalpracticesofwash-ingthedeadbodywerenotallowedduetorisksofspreadingthevirus,theysoughtto"unzipthebodybagfor[thefamily]fromadistancesotheycansee,andhav-ingmoreattentiontokindofwhatthefuneralprocesslookedlike,andsothenwecould,atleastasmuchaspossible,honoreachperson"(P21).
Frominitialcontactuntilafterdeath,actionstoup-holdthedignityofpatientsfacingdeathwerefelttobecriticallyimportant,evenamidsttheinherentcomplex-itiesofresponse.
Throughactsofcaring,respondingtosuffering,upholdingprivacy,andrespectingtraditions,participantsexpressedthattheidentitiesandindividualworthofeachdyingpersoncouldberealized.
BalancingcareprioritiesEffortsaimedateasingsufferingandupholdingdignityareenactedinabroaderhumanitariancontext,oneinwhichresourcesarefiniteandoftenscarce,andlifesav-ingremainstheprimaryfocus.
Asnotedabove,partici-pantsacceptedthisbroadunderstandingofpriorities.
Forexample,aparticipantexpressedthatinthecontextofthewarinSyria,"thosepatientswiththepalliativeneeds,unfortunately…theystarttofeelliketheyaresec-ondpriority"(P16).
AmoreextremeversionofthisprioritizationwasdescribedbyaparticipantinamasscasualtysituationfollowingviolentclashesinCentralAf-rica:"there'ssomanythatstillneedyourattentionthatwereallyhavenothingtoevenoffertothosethatwerenotgonnamakeit"(P19).
Anursestatedthat:Imean,obviouslyinabigdisaster,inabigmasscasualtyeventorareally,really,busycomplexconflict,theamountoftimethatpeopleareabletogivetopalliativepatientsisgoingtobelimited.
AndIthinkthat,unfortunately,that'sareasonabledecision…(P23)Whileacknowledgingtheneedtoprioritizelifesaving,severalparticipantsnonethelessdescribedtheprovisionofcaretodyingpatientsasanessentialobligationofjustice.
Aphysicianwhohadexperienceasapolicy-makerdescribeditthus:"…patientswhosimplyneeddecentcarefordying-youneed,youareobligedtocalculateandprovidere-sourcestoaccommodatethosepatients….
"(P14).
GivenHuntetal.
JournalofInternationalHumanitarianAction(2018)3:12Page6of13thesecommitments,participantssuggestedthathumanitar-ianhealthprofessionalsshouldmakeprovisionstoensurethatsuchcareispossible.
Forexample,anotherphysicianpolicy-makerrecommendedthatsomehealthcareresourcesshouldbededicatedtoaddressthesufferingofdyingpa-tientsevenduringtriagesituations,includingreservingpainmedicationforthesepatientsand:tokeepsomeresourceevensomepartofthe,ofthestaff…topayattentionandtoprovidethisbasiccaretopeoplewhowillnotbereceiving…life-savingtreatment:theywillprobablydie,theymaydie,butatleasttheyshoulddie…inarespectfulway,inadignifiedway,andasmuchaspossiblewithouttoomuchpainandwiththepresenceofsomebody.
(P10)Severalparticipantsexpressedthatitisimportantnottoextrapolatefromthemostacutesituationsofurgencyasarationalefornotaddressingsufferingorpromotingdignityforpatientsinotherhumanitariansettings.
Astheacuityofanemergencydecreases,aphysiciannotedthattherationaletolimithealthcaretoprimarilylifesav-ingefforts,withlimitedattentionavailabletorespondtootherneeds,"doesn'tstaytrue"(P18).
Moreover,adistinc-tionwasdrawnbetweenbasiccarethatattendstosuffer-inganddignityandamorecomprehensiveversionofpalliativecare,whichsomesawas"aluxury"(P2,P11)inacutehumanitariansettings.
Fundamentally,participantshighlightedwhattheysawasafalsedivideandtheneedformoreintegrationofcura-tiveandpalliativeapproaches.
Addressingthepossibilitythatthefocusonlifesavingwouldnotleaveroomforpalliativecareapproaches,aparticipantthuscalledforhu-manitarianstorejectachoicebetweenpalliativecareandcurativecare.
Heexpressedthathumanitariansshouldprovidelifesavingcareand"simultaneously…providees-sential,basichumancareto[patientswhowilldie].
Andit'snotoneortheother.
It'sweneedtocombinebothapproaches,andthisprobablyisasmallrevolutioninthewayweenvisageourroleinthefield.
"(P10).
Workingwithin,andresisting,systemicconstraintsParticipants'effortstoprovidepalliativecarewerecir-cumscribedbysystemicconstraintsinherenttohumani-tarianoperationsandtothewidercontextofglobalinequalityinhealthcareaccess.
Participantsidentifiedthedifferentwaysinwhichtheyengagedwithunfairsys-tems,andtheimpactthesedifferentwaysofengaginghadonthecaretheyprovidedpatients,andontheirownwell-beingascareproviders.
Participantsempha-sizedthatitwasfeasibletoaddressmanyneedsofdyingpatientsinhumanitariansettings.
Aphysicianwhohadworkedinthreesituationsofarmedconflictstatedthat"…fromahumancompassionperspective,somethingsthatpeopledieofarepainfulanduncomfortable.
Andwehavethetoolstolimitthatdiscomfortandweshouldusethem"(P23).
Variousfeaturesofhumanitarianpro-jectswereidentifiedasenablingsuchcare,includingstrongpartnershipswithlocalorganizations,havingclearguidanceandsupportiveleadership,andaccesstoopi-oidsandotherneededresources.
However,itwasmorecommonforsystemicfeaturesandarangeofbarrierstoconstrainhealthprofessionalsintheirresponsetothosewhoweredyingorlikelytodie.
Forexample,careop-tionsareoftenlimitedbylackofaccesstomaterialandhumanresources.
Participantsdescribedlackofaccesstopainmedications,especiallyopiates,aswellasequip-ment(e.
g.
,diagnostics,ventilators)andsupplies.
Short-agesofstaffwithskillsandtraininginpalliativecareorthepresenceofstaffwithskepticalorcontraryviews(betheylocalorexpatriatehealthprofessionals)werealsohighlightedasbarriers.
Whencoupledwithalackofclearpalliativecareorganizationalpolicyguidanceandclinicalguidelines,theseobstacleswerefurtherrein-forced.
Othersystemicfeatureswerealsoidentified.
Participantswereconcernedwhentheysawpatternsofneglectingsuffering.
Forexample,aphysicianfeltthatthistendencyreflecteda"tyrannyoflowexpectations"(P22)whichsheassociatedwithaformofimplicitra-cismandwhichresultedinhumanitarianorganizationsrespondinginadequatelytopainandsuffering.
Overall,participantsstressedthatthesechallengescanandshouldbeaddressedwithsustainedefforttoimproveaccessandthequalityofpalliativecareavailable.
Participantsframedmanyofthesefeaturesasunfairandasresultingfromand/orcontributingtowiderin-equalities.
Theydescribedcircumstancesasunjustatthegloballevel,suchasinequalitiesrelatedtowhichnationsbearthebruntoftheglobalrefugeecrisis(relativetotheirwealthandinfluence),orwhetheraparticularpatientwouldhavesurvivedtheirinjuriesiftheyhadoc-curredintheparticipant'shigherresourcedhomecoun-try.
Whilediscussingapatientwhodiedofaninfectedwound,aphysicianfromahigh-incomecountrynotedthat"Ithinkwefounditchallengingbecause…ifwe'dseenthisguypre-hospitalanywherein[homecountry],wewouldhavebeenabletodealwithlotsoftheseissuesquiteeffectively"(P17).
Anotherphysiciandescribedherdistress"performingtreatmentsthatIknewIcoulddowithlesspainandbettertolerabilityinabettersetting,butwasunabletodoatthattime"(P22).
Participantsalsodiscussedunfairnessinparticularcir-cumstances,suchasexpressingfrustrationwhenencoun-teringpatientsdyingfromconditionsthatcouldhavebeeneasilypreventedwithbetteraccesstobasichealthcare,andunfairnesswhencertainsubgroupswithinthelocalpopula-tionhadlessaccesstocare.
Severalparticipantsalsoidenti-fiedinequalitiesorinequitiesacrosshumanitarianprojects.
Huntetal.
JournalofInternationalHumanitarianAction(2018)3:12Page7of13Forexample,aphysiciandescribedhowtherewas"anunevensupplyofmedicationsacross"(P3)EbolaTreatmentCenters,includingmorphine.
Discussingthesamesitu-ation,anurseidentifiedthesourceoftheseinequalitiesasdifferentrulesamongsttheEbolaTreatmentCentersfun-dersandpartneringorganizations.
Sheworkedinacenterwheretherulesofapartneringorganizationprohibitedtheuseofmorphineandexpressedthat,asaresult,"therewasalotoffrustrationthatthingswerereallybadforthepa-tientsinourtreatmentcenters,andunfairlyso"(P21).
Participantsrespondedinavarietyofwaystosystemicconstraintsandtheinequalitiesandunfairnessthattheyengendered.
Insomesettings,participantsfelttheyneededtomakereasonableifdifficultcompromisesduetotheconstrainingnatureofthecircumstances.
Work-inginaninsecureandchaoticarmedconflictsettingwheretherewerefewhealthprofessionals,aphysicianreportedreluctantlymakingthedecisiontonotallowfamilytovisittheirdyinglovedonesinthehospital.
Theteamwas,however,abletoprovidepainmanagementdespitethelimitednumberofhealthcarestaff:Thesepeoplemaydiewithouttheirfamilymembersaroundthem,whichisobviouslynotideal.
Butinthosecases,Idothinkthat'sareasonablelimittotakeforsecurityreasons,forresourcereasons,forfunctionofthehospitalreasons.
So,thatwouldbeacompromisethat'smade,suboptimalstaffing,perhaps,andsuboptimalpsychosocialcare,butnevertheless,abasicminimumintermsofpainmanagement.
(P23)Participantsalsodescribedthattheyandtheircol-leaguessometimesneededtoadjusttheirperspectiveinhumanitariansettings.
AphysicianfromNorthAmericaexpressedthatexpatriatehealthprofessionalsneedtoaccept"thatwecan'tdotherewhatwecando[inhomecountry]"(P15).
Shealsodescribedhowshehadneededtolearntobecomemoreacceptingofthedecisionsmadebypatientsandtheirfamilies.
Shereportedthatitwasdifficultforhertounderstandamother'sdecisionprocess:wecan'tevenconceiveofit,wecan'tevensortouthowshe'smakingherdecisions,ifshe'sgoingtostaywiththatchild[inthehospital]orshe'sgoingtogohomeandlookaftertheothereightonesthatdon'thaveanybodylookingafterthembecausetheirDadhasalreadybeenkilledinthewar.
(P15)Humanitarianhealthprofessionalsreacttothesediffi-cultiesinvariedways,sometimesgoingbeyondadjustingperspectives,tolosingperspective.
Aphysicianreportedthattheaustereanddifficultcircumstancesofhumani-tarianemergenciescanleadexpatriatehealthprofessionalsto"turnpeopleinto'other',turnoffyouremotionsandjustbelike,'holdthemdownandwe'lldothis'"(P22).
Sheassertedthattakingthisperspectivemustbeactivelyresisted;regardlessofthecircumstancesinwhichpeopleareliving,theyshouldbetreatedwithrespectandbepro-videdcaretorelievetheirsuffering.
StoriesofresponsivenessandadaptationinthecontextoftheWestAfricanEbolaepidemic,forexample,high-lightwaysthatteamsbecamemoreadeptatworkingwithinandpushingagainstconstraints,includingbychallengingpoliciesandinnovatingtobetteraddressneedsofpatientsinacontextofextremelyhighmortal-ityrates.
Aparticipantdescribedthathisteam"gotalotbraverandalotmoreboldwithhowweweretreatingpeopleandgivingthemalotmoreattentionoralotbet-tercare"(P11)astheEbolaoutbreakprogressedandtheydevelopedmoreknowledgeandskillformanaginginfectioncontrolriskswhileprovidingbetterandmorecompassionatecaretopatients.
Inothersettings,emer-genttechnologieswereidentifiedasprovidingsupporttoovercomeobstaclestocare.
Forexample,telemedicinewasidentifiedbytwoparticipantsasameanstoaccessexpertsinpalliativecareinsituationswheretheteamlackedsuchexpertise.
Inanothercontext,aphysiciandescribedhow,evenwhenopioidswerenotavailable,ultrasound-guidednerveblockscouldbeusedtoprovideeffectivepainrelief.
Advocacywasalsodescribedasanimportantpositiveresponsetoobstaclesandconstraints.
Thismightoccuratmultiplelevels:withintheteam,intheorganization,andinternationally.
Aphysicianpolicy-makerexpressedthathumanitariansshould"advocate.
.
.
forpalliativecareinhumanitariancrisestobeabasichumanright…Itshouldbethenorm.
Itshouldbeahumanrightandthenorm"(P1).
Manyparticipantssuggestedthathumani-tarianscanadvocatewithintheirorganizationforbetteraccesstoresourcesneededforimprovingbothcurativeandpalliativecare.
Aphysicianexpressedthatthesedualadvocacyeffortsgo"hand-in-hand"(P3).
Discussingthemanyburnedpatientsforwhomherteamwasunabletoprovideadequatepainmedication,aphysicianexpressedregretthatshehadnotbeenmoreforcefulinheradvo-cacyefforts,sayingthat"IfIhadbeenalittlebitmoreontheballaboutit,Icouldhavekickedupabiggerstink"anddemandedmorphineandketaminebemadeavailable(P22).
Thesevariousresponsesultimatelyre-flecttheweightofresponsibilityandmoralobligationparticipantsexperiencedinhowtheyrespondedtopa-tientsintheircarewhoweredying.
BearingtheweightofresponsibilityThenarrativesconveyaprofoundweightofresponsibil-ityfeltbytheparticipants.
Instoriesofpalliativecare"donewell"inahumanitariansetting,thisweightfeltHuntetal.
JournalofInternationalHumanitarianAction(2018)3:12Page8of13liftedoratleastlighterontheshouldersofparticipants.
Manyparticipantscouldnotthinkofacasewherepal-liativecarewasdonewell,butamongstthosewhocould,theirexperiencewasasourceofdeepsatisfaction.
Pro-vidingeffectivepalliativecare"…allowsthehealthcareworkerstofeelthattheyarecontributingandtheyhaven'tfailed"(P6).
However,evenwhencarewasdonewell,theseencounterscouldstillhauntparticipantsasmorallyandexistentiallysignificant.
Forexample,anursewhohadworkedinanEbolaTreatmentCentredescribed"alittlegirl,Ithinkabouttheageofnine,andwhocalledme,'Unclecanyouholdmyhand',andbe-causeIknewthatwecouldsitdownandtalktothem,so–whichIdid,andonceIheldherhand,shedied…andso,for-formany,manymonths,evenwhenIcame[home],Icouldstillfeelthattouch…Icouldstillfeel-hearthatvoice"(P20).
Thisexperiencestayedwithhim,andhedescribeditasonefactorinhisseekingpsycho-logicalsupportafterreturningfromhisfieldmission.
Situationswhichparticipantscharacterizedascarenotdonewellwereoftenassociatedwithparticularlyheavyemotionalstrain.
Somedescribedfeelingsofhavingfailedcertainpatients,andthesesituationsgaverisetodistressandfeelingsofguiltorregret.
Thisresponsewasparticularlyacutewhenparticipantsfeltthattheywereimplicatedinasituationthatwasprofoundlyandin-escapablyunjust.
Forexample,aphysiciandescribedhow"I'veliterallywatchedhundredsofbabiesseizetodeathandit'sjustaterrible…ButIdidn'thaveawayofkeepingthemcomfortable,andlettingthemdieinawarm,comfortableplaceandthatreallyhauntsme"(P22).
Feelingsomehowcomplicitinwhatwasoccur-ring,shewentontosaythat"Idon'tbelieveinhell,butIkindofthinkthereisaspecialplaceinhellforme.
"Especiallydifficultwerecircumstanceswhenpatientswhoweredyinginpainwereturnedawayfromcare,asituationwhichcanbe"devastatingemotionally"(P10)forhumanitarianworkers:"…itgoesagainsteverythingthatyou–asahealthcareworker,asahumanitarian,everything–todothattoahumanbeing,youknowthey'renotgonnamakeitandjustputthemaside,itwas–terrible(P19).
"Inadditiontostoriesofnotprovidingcaretodyingpatientsorofinsufficientlyaddressingsymptomsordig-nityfordyingpatients,participantsalsoreporteddistressaboutprovidingtreatmentthatprolongedthesufferingofadyingpatientwhentheparticipantfeltthatcareshouldhavebeenfocusedonpalliationbutwasnot,duetosecurityconcerns,orattheinsistenceofthefamilyorotherhealthcareprofessionals.
Participantsdescribedstrategiesthathelpedthemcarrytheweightofresponsibility.
Theyemphasizedtheimportanceofsharingtheweightwithtrustedcol-leagues,throughdiscussionandcollaborationwithinteams.
Closeteamrelationshipsthatincludedsharedplansforrespondingtotheneedsforpalliationwerede-scribedasimportant.
Aphysiciandescribedhowasharedplanallowedhisteamtofeel"comfortablewithwhateverwasgoingtohappen"(P15).
Otherstalkedaboutredirectingtheirfeelingsofnothavingprovidedsufficientcaretosomepatientsintoactionaimedathelpingotherpatients,includingthroughadvocacy.
Incontrast,severalparticipantsdescribedactivelytryingtoforgetcertaintroublingexperiences.
Organizationalstrategiesincludingsupportanddebriefingwerealsoidentifiedasvaluable.
Anursedescribedthelackofongoingpsychologicalsupportforhealthprofes-sionals,especiallynationalstaff,providingcareinEbolaTreatmentCentersasoneofthe"bigfails"ofhisorganization(P11).
Healsoidentifiedtrainingpriortodepartureasanimportantcomponentforhelpingpeopleanticipatethechallengesoffacingsuffer-ing,dying,anddeath,andbetterpreparingforthem.
Severalparticipantsreportedstrugglingwiththeirexperiencesofprovidingornotprovidingcaretodyingpatientsinahumanitariancrisis,evenaftertheirreturnhome.
Forexample,anursewhohadrespondedtotheEbolaoutbreakstatedthat:yes,itwasheavy…[S]omeofthethingsIdid,theydidn'tactuallycauseanyproblemswhileIwasthere,butwhenIcame[home],Icouldn'tsleep.
Itaffectedmysleep,myeating,evengoingtowalk.
Icouldn'thaveashowerforsometimesoitwasheavywhenIcameback…Ihadtoreceive–Igotsupport…psychotherapy,forIthinkupto6monthsor8months…(P20)Anotherparticipantreportedasimilarpattern,statingthat:Youthinkaboutthemwhenyoucome[home].
Youdon'thavetimetoprocessanything[inthefield],becauseyou–you'resooverwhelmedbythesituation,youdowhatyoucaninthatmoment,andyouhavetomoveon,becausethenextdaycouldbringtheexactsamething.
Soyoucanonlyprocessforyourownmentalhealthwhat'srightinfrontofyou.
Untilyoucomehome,atleast…andthenyoustarttokindof–reallythinkaboutwhatyoudid,orwhatyoudidn'tdo,and–sometimesthere'sabig–…discordanceofwhat–yourideals,andwhatyouactuallydid…theyjustaren'tmeetingupandit'sahugementalstrugglethen.
(P19)Fortheseparticipants,theweightofresponsibilitydidnotliftaftertheyreturnedtotheirhomecountries.
TheyreportedlingeringimpactsoftheseexperiencesofHuntetal.
JournalofInternationalHumanitarianAction(2018)3:12Page9of13respondingtotheneedsofpatientswhoweredyingorlikelytodieinhumanitariancrises,orofbeingunabletorespondtotheseneedsinwhattheyfeltwastherightway.
DiscussionParticipantsinourstudydescribedalleviatingsuffering,upholdingdignity,andaccompanyingindividualswhoaredyingorlikelytodieasobligationsofhumanitarianhealthprofessionalsandhumanitarianorganizations.
Notprovidingcaretosuchindividualsinhumanitariancriseswasdescribedandexperiencedbythemajorityasethicallywrong.
Atthesametime,seekingtoprovidepalliativecarefordyingpatientswaschallenging.
Inten-tionstoprovidesuchcarecouldbeseverelyconstrainedbylimitedresourcesavailableinthefieldorataparticu-larmomentinacrisis.
Thedominantethicofprioritiz-inglifesavinginthefaceoflimitedresourcesreinforcedlimitedpreparednessforandallocationofhealthcareresourcestowardthosepatientswhowerenotexpectedtosurvive.
Anawarenessofculturaldifferencesinend-of-lifepractices,expectations,andnorms(Gaudioetal.
2013;Gyselsetal.
2011;Hajjaretal.
2015)addedanotherlayerofcomplexitytothematterforprovidersworkingasexpatriatesincrisissettings.
Weproposethesescenariosanddecisionscameacrossasethicallytroublingtoparticipantsbecauseofthedegreeofsuffer-ingexperiencedbydyingpatients,butalsobecauseofthewaythesesituationshighlightedexistinglimitsforhealthprofessionalsrespondinginsituationsofhumani-tariancrisis.
Respondingtotheneedsofdyingpatientsinhumani-tariancrisesisheavilyfreightedwithethicalimplications,especiallygiventhepossibilityofdiscordancebetweenhumanitarians'valuesandwhatactionsseempossibleinahumanitariancrisis,arealitythatDeWaal(2010)hasdescribedasthetragedyofhumanitarianaction.
Thesesituationsalsointersectwithideasaboutwhatitmeanstobeahumanitarian,thedutiesofhealthprofessionals,andevenwhatitmeanstobeahumanbeing.
Encoun-terswithpatientswhoarelastinlinewithinatriagesystemthatprioritizestherescueandprotectionoflifearerememberedwithasenseofparticularimportance.
Forafewparticipants,decidingtoreservescarcehealth-careresourcesforthosepatientswhoareexpectedtosurviveaffirmstheirhumanitarianidentityandresponsi-bility,assuchdecisionslinktotheweightofhavingtodeterminehowtoallocatescarceresources.
Formost,suchchoicesleftparticipantsdeeplytroubled.
Expressedasguilt,outrage,ordistress,thesefeelingsarethemoralresidue(WebsterandBaylis2000)ofbeinginvolvedincompromisedcarethatgratesagainsttheirsenseofdoingthe"right"or"human"thingandpotentiallyresultinmoraldistress(Jameton1993).
Themoralworldsofhumanitarianhealthcareprofes-sionalsofwhichwecaughtaglimpsethroughthisstudyreflectandreaffirmthegoalsofhumanitarianactiontosavelives,alleviatesuffering,andmaintainhumandignity(SphereProject2011a).
Accordingtoourparticipants,thereluctancetoincludepalliativecareinhumanitarianhealthcareistheresultoftheoverarchingfocusonlifesav-ingandrescueinthiscontext,aviewwhichequatesdeathas(always)ahumanitarianfailure.
Recentcommentatorshavepushedforacceptancethatnotallpatientscanbesavedinhumanitariansettingsandthatthefailureliesinnottakingstepstoaddresssufferinganddignityforthosewhowillsuccumbtoinjuryordiseaseintheseset-tings(SmithandAloudat2017).
Participantsgenerallyexpressedhopethatmorecouldbedonefordyingpatientsinhumanitariancrises,inparticularbyinte-gratingcurativeandpalliativeapproachestocare,whilealsoacknowledgingsystemicandculturalchallengestodoingso(Huntetal,2017).
Theseconddraftoftheup-datedSpherehandbookendorsestheneedtoaddresssuf-feringandpainreliefforallpatients,includingpeoplewhoareexpectedtodie,andadvocatesforintegrationofpalliativeandcurativeapproaches(SphereProject2017).
Alongwithjusticeinaccesstocare,compassionstandsoutasanunderlyingethicalcommitmentinthepartici-pants'narrativesofcaringforpatientswhoaredyingorlikelytodie.
Whileitcouldbearguedthatallcareis(orshouldbe)compassionate,anumberofactionswereidentifiedbyparticipantsasmeaningfulmomentsbe-causeofthewaythesebroughtanon-medical,relationalcommunionwithpainandrecognitionofsharedhuman-ityintothehumanitarianpalliativesetting.
Thesein-cludedtouch,simpleconversation,andsharedprayerswithpatientsinthemomentspriortodeath.
Fundamen-tally,participantsappearedtoidentifywiththeuniver-salityofthehumanconditionsofpain,suffering,anddeath,andfeltitdemandedanempathetic,holistic,andtangibleresponse.
Itisinthisrecognitionandresponsetothehumanityoftheotherthatcompassionappearstoconnecttotheupholdingofdignityinparticipants'moralworlds.
Theconceptofdignityiswidelyusedinarangeoffields,yetitsdefinitionremainscontested.
Indeed,somebioethicsscholarshavearguedthatitisreplaceablebymorepreciseconceptssuchasrespectforpersonsandautonomy,evencallingita"uselesscon-cept"(Macklin2003).
Barclay(2018)hascounteredthisview,drawingonscholarshipfrompoliticalphilosophy,tosuggestthatthedistinctivecontributionofdignityisinemphasizingandembodyingequalmoralworth.
Thisperspectiveappearsconsistentwithourparticipants'useoftheterm,andtheiremphasisondignifieddeath,inclu-dingdyingpatientsnotfeelingabandonedortreatedaslessthanhuman.
Thisperspectivereflectsarelationalqualityofdignity.
ItisalsoresonantwiththebroaderHuntetal.
JournalofInternationalHumanitarianAction(2018)3:12Page10of13discussionofdignityinhumanitarianaction,whereitisdirectlyassociatedwithactsofrespectforpersonsaffectedbycrises(SphereProject2011b),andwithconceptionsofUbuntuinAfricanethicalthought(Behrens2013).
Behindthenarrativesofsomeparticipantswasacon-cernwithentanglementinsituationsofpoliticalandsocialinjustice.
Inthissense,providingpalliativecare,"becausethereisnothingelsetooffer,"isassociatedwithquestionsaboutbeingentangledinthemanufacturedcircumstancesthatprecipitatedsufferinganddeath.
Itreflectsabroaderconcernforaidworkerswho,adheringtothehumanitarianprincipleofneutrality,areconsciousthatadvocatingagainstinjusticecouldmeantheyloseaccesstothecommunityandthosewhoneedcaremost(Terry2002).
Differentformsofcomplicityinhumani-tarianactionhavebeenidentified,andattentionhasbeendirectedtodistinguishingthemfromrelatedethicalconcepts(LeporaandGoodin2013).
Amongstourpar-ticipants,severalexperiencedfeelingsofbeingcomplicitonamoreindividuallevel.
Participantsdescribedmo-mentswhentheyortheircolleaguesfailedtodoenoughasthemomentsthatcontinuetohauntthem.
Forex-ample,participants3and5expressedadeepandlinger-ingremorseforpatientswhotheyfeltweredeniedadignifieddeath,asahuman,duetoinactionontheirpart.
Theymayhavebeenunabletotakeamomenttospeakwiththepatient,toholdtheirhand,ortellthemwhatwashappening.
Feelingsofhavingfailedtoad-equatelyattendtopatientswithpalliativeneedsinhumanitariancontextsengendermoralstressthatturnsintomoraldistresswhenthecasesarecompounded,andindividualsfeeltheyhavecompromisedsignificantper-sonalandprofessionalvalues.
Lingeringeffectsofthissenseofcomplicityremainwithactorsasmoralresiduewhichmight,inturn,causethemtofeelhelpless,dis-trusttheirownactions,and,turnedinward,leadtocom-passionfatigueandburnout(Horningetal.
2017).
Thestudyfindingsalsodrawattentiontotheimport-anceoftrainingandpreparationintheareaofpalliativecareinhumanitariansettings.
Toeffectivelyrespondtotheneedsofdyingpatients,humanitarianhealthcareprofessionalsrequiretrainingandskills,aswellasguid-anceonhowtoprovidepalliativecareinhumanitariancrisissettings.
Ourparticipantsidentifiedexperienceswithpatientsandfamiliesfacingdyinganddeathasdeeplyaffecting.
However,manydescribedfeelingillequippedorunsupportedtorespondeffectivelytotheneedsofthesepatients,andthemoraldistressthiscreatedforthematthetime,andoftenlongafter.
Thisincludedseveralforwhomtheirexperiencesimpactedtheirmentalandemotionalwell-beingtoanextentthatmayhavejeopardizedtheirabilitytocontinueinhu-manitarianwork.
Formostparticipants,expressionsoftheethicalim-perativesofrespondingtosufferingandupholdingdignitywerealmostalwayscoupledwitharecognitionofthepragmaticneedfororganizationalandoperationalinclusionfortheresponsetobeconsistentandeffective.
Currently,thereareseveralongoinginitiativesthatareseekingtoaddressgapsintrainingandguidance.
Forexample,MédecinsSansFrontièreshasdevelopedapediatricpalliativecareguideline(SmithandAloudat2017)andMédecinsDuMondeisimplementingapilotprojectonpediatricpalliativecareintheDemocraticRepublicoftheCongo(seeMédecinsduMonde2016).
Theseareencouragingdevelopmentsandmoveindirec-tionsproposedbyparticipantswhoidentifiedorganizationaleffortstobuildaspaceforinclusionofpalliativecareases-sentialforengagingthecomplexcontextualissuesauthen-ticallyandconsistently.
Thecontextofhumanitariancrisescreatedneedsfortriageandprioritizingcarethatwereoftenunique.
Further,therewasrecognitionthatorganizationalpalliativecarestandardswouldrequiresignificantadaptationtolocalperspectivesgiventheculturalspecificitiesofthenatureofsufferinganddeath.
Differencesbetweenlocalandexpatriatepro-viders'viewsonsufferingorwhenandhowtoacknow-ledgetreatmentfutilitywerefrequentlycited.
Itwasalsorecognizedthatcareforthosefacingdeathwouldneedtoincludefamiliesandcommunitiesexplicitly.
Furthermore,differentformsofhumanitariancrises(e.
g.
,conflict,suddenonsetdisaster,epidemic)willshapeneedsandpossibilitiesforpalliativecareprovision,andthesedifferencesshouldbeaccountedforinguidelinesandtraining.
Onahigherlevel,itwashopedthatinclusionwouldalsobereflectedineffortsbythewiderhumanitariancommunitytoadvocateonissuessuchasaccesstoessentialpalliativemedicinesespeciallyopiatesandtheinternationalandnationalregulatoryandpolicyissuesthatarise.
AccordingtotheWorldHealthOrganization,"onlyabout14%ofpeoplewhoneedpalliativecarecur-rentlyreceiveit"(WHO2018).
Despiteglobalstatementsthatpalliativecareisahumanright(InternationalChil-dren'sPalliativeCareNetwork2008,WHO2018)andacorecomponentofuniversalhealthcoverage(WHO2018),accesstosufficientpainreliefisdeplorablylowinLMICs,especiallyamongstchildren(Knauletal.
2018).
ThisbackgroundsituationdirectlyaffectsaccesstopainmanagementinhumanitariancrisesinLMICs,especiallywherelaworpolicylimitorpreventtheimportationofopioids.
Humanitarianactorshaveexpressedacommit-menttoadvocate(NickersonandAttaran2012)andrallyinternationalorganizations,governments,policy-makers,andhealthcareproviderstotakethe"necessarystepstoensurethatallpatientsinneedhaveaccessto"essentialmedicinesforpalliativecare(DeLimaetal.
2007).
ItwasHuntetal.
JournalofInternationalHumanitarianAction(2018)3:12Page11of13feltthatadvocacybyhumanitarianproviderswouldfur-thertherecognitionandinclusionofpalliativecareinna-tionalandlocalhealthsystemsglobally.
Concernswereraisedaboutintroducingcarethatcouldnotbesustainedoncehumanitarianresponsehasended,butthiswasoffsetwiththepotentialopportunityforcapacitybuildingandhealthsystemsstrengthening.
Inresponsetotheirexperiencesinhumanitariancaresettings,manyofourparticipantswereledtoadvocateatdifferentlevelsfortheexplicitinclusionofpalliativecareinhumanitarianresponse.
Atthesametime,itiscrucialtoensurethatpalliativecareisnotseenasareplacementforcurativecarewhereitispossibletoprovideit(SmithandAloudat2017).
ScopeandlimitationsofthestudyThispaperfocusesontheexperiencesofexpatriatehealthprofessionalsrespondingtotheneedsofpatientswhoaredyingorlikelytodieinahumanitariancrisis.
Thisisanimportantperspective,butstillalimitedangleofview.
Investigatinghowpatients,theirfamilies,andlocalcommunitiesandhealthprofessionalsviewandexperiencethesesituationsisessentialforbetterunder-standingwhatisatstakeandforwhom.
Ourlargerresearchprojectinvolvesin-depthfieldresearchinhu-manitariansettings,includingperspectivesfrompatientsandtheirfamilies.
Theseinquirieswillprovideadditionalvantagepointsforunderstandingthistopic.
Severallimita-tionsarerelevanttotheanalysispresentedhere.
Ourpur-posivesamplingstrategywasonlypartiallysuccessful.
MostoftheparticipantswereEuropeansorNorthAmericanswhoprimarilyworkedwiththelargestoftheinternationalNGOs.
Thisdoesnotreflectthewiderangeofnationalitiesofexpatriatehumanitarianprofessionals,orthespectrumofhumanitarianorganizations,andhasundoubtedlyshapedtherangeofexperiencesandethicaloutlooksoftheparticipants.
ConclusionDeathanddyingareinescapableinhumanitariancrises.
Increasedattentionisbeingdirectedtowardquestionsrelatedtowhyitisimportantforhumanitarianorganiza-tionstorespondcompassionatelyandinajustmannertotheneedsofthesepatients,andhowtheyoughttoplanfor,implement,andassesstheseefforts.
Thestudyreportedhereprovidesimportantinsightintothemoralexperiencesofhumanitarianhealthprofessionalswhoencountersuchpatientsandhighlightssomeimportantaspectsofwhatisatstakeinthesesituations.
Theirper-spectivesspeaktoboththeessentialimportanceandcomplexitiesofcontextuallyappropriatepalliativecare.
Wehopethatitwillalsoencourageandsupportfurtherdialogueinthehumanitariansectoronthistopic.
Itiscrucialthathumanitarianhealthcareprofessionalsareprepared,supported,andresourcedinwaysthatenablethemtoattendtothesufferingandupholdthedignityofsomeoftheirmostvulnerablepatients:individualswhoaredyingorlikelytodieinhumanitariancrises.
Endnote1Atthetimeofwriting,aseconddraftoftherevisionwasavailableonline(SphereProject2017).
AbbreviationsLMICs:Low-andmedium-incomecountries;NGO:Non-governmentalorganization;WHO:WorldHealthOrganizationAcknowledgementsWearegratefultothestudyparticipantsforsharingtheirexperienceswithus,toRachelYantziforherassistancewithformattingthemanuscript,andtotheothermembersofourresearchteam,LaurieElit,LyndaRedwood-Campbell,OliveWahoush,CorinneSchuster-Wallace,ErynnMonette,MadelineMcDonald,RossUpshur,andJhalokRonjanTalukdar,fortheircontributionstoourbroaderresearchstudy.
FundingTheresearchpresentedinthisarticlewassupportedbyagrantfromElrha'sResearchforHealthinHumanitarianCrisesprogramme(Project#19775:Aidwhenthereis"nothinglefttooffer":Astudyofethicsandpalliativecareduringinternationalhumanitarianaction).
TheResearchforHealthinHumanitarianCrises(R2HC)programmeaimstoimprovehealthoutcomesbystrengtheningtheevidencebaseforpublichealthinterventionsinhumanitariancrises.
Visitwww.
elrha.
org/work/r2hcformoreinformation.
TheR2HCprogrammeisfundedequallybytheWellcomeTrustandDFID,withElrhaoverseeingtheprogramme'sexecutionandmanagement.
MatthewHuntissupportedbyaResearchScholarAwardfromtheFondsdeRechercheduQuebec-Santé,andLisaSchwartzissupportedbytheArnoldLJohnsonChairinHealthCareEthics.
Authors'contributionsMH,AC,andKBdevelopedtheinitialideaforthismanuscript.
MHwrotethefirstdraft,andallauthorsmadesubstantialcontributionsasthepaperwasrevised.
SdLandENconductedinterviewswithparticipants.
GKandACconductedinitialcodingofinterviewtranscripts.
Allauthorsreadtheinterviewtranscriptsandparticipatedinthedataanalysis.
Allauthorsapprovedthefinalversionofthemanuscript.
Author'sinformationMatthewHuntisanassociateprofessorattheSchoolofPhysicalandOccupationalTherapyofMcGillUniversityandanassociatememberoftheBiomedicalEthicsUnit.
Heconductsethicsresearchintheareasofglobalhealthandrehabilitationandco-leadstheHumanitarianHealthEthicsRe-searchGroup(humanitarianhealthethics.
net).
AniChénierisananthropologistwhoseworkexploresthewaysmortuaryandcommemorativematerialcultureenactandtransformsocialimaginaries.
SheisaresearchcoordinatorwiththeHumanitarianHealthEthicsResearchGroupatMcMasterUniversity.
KevinBezansonisapalliativecareconsultantfortheNorthwesternOntarioregionandbasedinThunderBay,Ontario,Canada,withclinical,research,andprogramdevelopmentexperiencemainlyinMalawiandEthiopia.
ElyséeNouvetisamedicalanthropologistandanAssistantProfessorintheSchoolofHealthStudies(GlobalHealth)atWesternUniversityinLondon,Ontario.
Herworkfocusesonlivedexperiencesoftrans-nationalaidandcare.
Sheisaco-leadoftheHumanitarianHealthEthicsResearchGroup.
CarrieBernardisafamilyphysicianandpalliativeleadfortheQueenSquareFamilyHealthTeaminBrampton,Ontario.
SheistheAssociateProgramDirectorofthePostgraduateFamilyMedicineprogramattheUniversityofTorontoandamemberoftheHumanitarianHealthEthicsResearchGroup.
SonyadeLaatisascholarofhistoriesofhumanitarianphotography.
CurrentprojectsincludephotographsofrefugeesfromtheFirstWorldWar,thevisualarchivesoftheCanadianInternationalDevelopmentAgency,andprojectsonphoto-basedoralhistoriesofhumanitarianaction.
GauthamKrishnarajisaresearchassistantwiththeHumanitarianHealthEthicsResearchGroupatMcMasterUniversity.
HeiscurrentlydeployedasanAgaHuntetal.
JournalofInternationalHumanitarianAction(2018)3:12Page12of13KhanFoundationCanadaInternationalYouthFellow,supportingthehealthandeducationinitiativesoftheMadrasaEarlyChildhoodProgram—Kenya.
LisaSchwartzisaprofessorintheDepartmentofHealthResearchMethodsandImpact(HEI)atMcMasterUniversityandanassociatememberoftheDepartmentofPhilosophy.
SheistheArnoldLJohnsonChairinHealthCareEthicsandisaco-leadoftheHumanitarianHealthEthicsResearchGroup.
LisaisalsoamemberoftheMédecinsSansFrontièresEthicsReviewBoard.
CompetinginterestsTheauthorsdeclarethattheyhavenocompetinginterests.
Publisher'sNoteSpringerNatureremainsneutralwithregardtojurisdictionalclaimsinpublishedmapsandinstitutionalaffiliations.
Authordetails1SchoolofPhysicalandOccupationalTherapy,McGillUniversity,845SherbrookeStreetWest,Montreal,Quebec,Canada.
2CentreforInterdisciplinaryResearchonRehabilitation,Montreal,Quebec,Canada.
3HumanitarianHealthEthicsResearchGroup,McMasterUniversity,1280MainStreetWest,Hamilton,Ontario,Canada.
4NorthernOntarioSchoolofMedicine,LakeheadandLaurentianUniversities,ThunderBayRegionalHealthSciencesCentre,980OliverRoad,ThunderBay,Ontario,Canada.
5SchoolofHealthStudies,WesternUniversity,1151RichmondStreet,London,Ontario,Canada.
6DepartmentofCommunityandFamilyMedicine,UniversityofToronto,Toronto,Canada.
7DepartmentofFamilyMedicine,McMasterUniversity,Hamilton,Canada.
8DepartmentofHealthResearchMethods&Impact,McMasterUniversity,1280MainStreetWest,Hamilton,Ontario,Canada.
Received:10April2018Accepted:27June2018ReferencesBarclayL(2018)Dignitarianmedicalethics.
JMedEthics44(1):62–67.
https://doi.
org/10.
1136/medethics-2017-104467BehrensKG(2013)TowardsanindigenousAfricanbioethics.
SAfrJBioethLaw6(1):32–35DeLimaL,KrakauerEL,LorenzK,PraillD,MacDonaldN,DoyleD(2007)Ensuringpalliativemedicineavailability:thedevelopmentoftheIAHPClistofessentialmedicinesforpalliativecare.
JPainSymptomManag33(5):521–526DeWaalA(2010)Thehumanitarians'tragedy:escapableandinescapablecruelties.
Disasters34(s2):s130–s137.
https://doi.
org/10.
1111/j.
1467-7717.
2010.
01149.
xElrha(2017)Takepartinthepalliativecareinhumanitarianactionsurveynow.
http://www.
elrha.
org/news/take-part-palliative-care-humanitarian-action-survey-now/.
Accessed13Mar2018GaudioFD,HichenbergS,EisenbergM,KerrE,ZaiderTI,KissaneDW(2013)Latinovaluesinthecontextofpalliativecare:illustrativecasesfromthefamilyfocusedgrieftherapytrial.
AmJHospPalliatCare30(3):271–278GiannouC,BaldanM(2009)Warsurgery:workingwithlimitedresourcesinarmedconflictandothersituationsofviolence,vol1Availableviahttps://www.
icrc.
org/en/publication/0973-war-surgery-working-limited-resources-armed-conflict-and-other-situations-violence.
Accessed20June2018GyselsM,PellC,StrausL,PoolR(2011)Endoflifecareinsub-SaharanAfrica:asystematicreviewofthequalitativeliterature.
BMCPalliatCare10(1):6HajjarRR,CharalambousHA,BaiderL,SilbermannM(2015)Internationalpalliativecare:MiddleEastexperienceasamodelforglobalpalliativecare.
ClinGeriatrMed31(2):281–294HorningJ,SchwartzL,HuntM,Williams-JonesB(2017)"Ifyouletitgettoyou…":moraldistress,ego-depletion,andmentalhealthamongmilitaryhealthcareprovidersindeployedservice.
In:MesselkenD,WinklerD(eds)Ethicalchallengesformilitaryhealthcarepersonnel:dealingwithepidemics.
Routledge,London,pp71–91HumanitarianHealthEthicsResearchGroup(2018)Palliativecareinhumanitarianresponse.
https://humanitarianhealthethics.
net/home/research/hhe-research-studies/pall-iphc/.
Accessed13Mar2018HuntM,BezansonK,BernardC(2017)Makingspaceforpalliativecareinhumanitarianaction:Reflectionsonobstaclestotheintegrationofpalliativecareapproachesinhumanitarianhealthcare.
Elrha.
http://www.
elrha.
org/r2hc-blog/making-space-palliative-care-humanitarian-action-reflections-obstacles-integration-palliative-care-approaches-humanitarian-healthcare.
Accessed13Mar2018HuntMR,CarnevaleFA(2011)Moralexperience:aframeworkforbioethicsresearch.
JMedEthics37(11):658–662InternationalChildren'sPalliativeCareNetwork(2008)TheICPCNcharterofrightsforlifelimitedandlifethreatenedchildrenhttp://www.
icpcn.
org/icpcn-charter/.
Accessed22Mar2018JametonA(1993)Dilemmasofmoraldistress:moralresponsibilityandnursingpractice.
AWHONNSClinIssuesPerinatWomensHealthNurs4(4):542–551KleinmanA(1999)Moralexperienceandethicalreflection:canethnographyreconcilethemAquandaryfor"thenewbioethics".
Daedalus128(4):69–97KnaulFM,FarmerPE,KrakaeurEL,DeLimaL,BhadeliaA,JiangKweteX,Arreola-OrnelasH,Gómez-DantésO,RodriguezNM,AlleyneGAO,ConnorSR,HunterDJ,LohmanD,RadbruchL,delRocíoSáenzMadrigalM,AtunR,FoleyKM,FrenkJ,JamisonDT,RajagopalMR,onbehalfoftheLancetCommissiononPalliativeCareandPainReliefStudyGroup(2018)Alleviatingtheaccessabyssinpalliativecareandpainrelief—animperativeofuniversalhealthcoverage:theLancetCommissionreport.
Lancet391(10128):1391–1454LamontagneF,FowlerRA,AdhikariNK,MurthyS,Brett-MajorDM,JacobsMetal(2018)Evidence-basedguidelinesforsupportivecareofpatientswithEbolavirusdisease.
Lancet391(10121):700–708LeporaC,GoodinRE(2013)Oncomplicityandcompromise.
OxfordUniversityPress,OxfordLincolnYS,LynhamSA,GubaEG(2011)Paradigmaticcontroversies,contradictions,andemergingconfluences,revisited.
In:DenzinNK,LincolnYS(eds)TheSagehandbookofqualitativeresearch,4thedn.
Sage,LosAngeles,pp97–128MacklinR(2003)Dignityisauselessconcept.
BMJ237:1419.
https://doi.
org/10.
1136/bmj.
327.
7429.
1419MarstonJ,DeLimaL,PowellRA(2015)Palliativecareincomplexhumanitariancrisisresponses.
Lancet386(10007):1940MédecinsDuMonde(2016)Soinspalliatifspédiatriques:Quandguérirn'estpluspossible,toutn'estpasterminé.
https://medecinsdumonde.
ch/activites/spp/le-projet/.
Accessed13Mar2018NickersonJW,AttaranA(2012)Theinadequatetreatmentofpain:collateraldamagefromthewarondrugs.
PLoSMed9(1):e1001153NouvetE,SivaramM,BezansonK,KrishnarajG,HuntM,deLaatS,SangerS,BanfieldL,EscobioRodriguezPF,SchwartzLJ(2018)Palliativecareinhumanitariancrises:areviewoftheliterature.
IntJHumanitarianAction3(5).
doi:https://doi.
org/10.
1186/s41018-018-0033-8PowellRA,SchwartzL,NouvetEetal(2017)Palliativecareinhumanitariancrises:alwayssomethingtooffer.
Lancet389:1498–1499.
https://doi.
org/10.
1016/S0140-6736(17)30978-9SchneiderM,PautexS,ChappuisF(2017)WhatdohumanitarianemergencyorganizationsdoaboutpalliativecareAsystematicreview.
MedConflSurviv33(4):263–272.
https://doi.
org/10.
1080/13623699.
2017.
1409167SmithJ,AloudatT(2017)Palliativecareinhumanitarianmedicine.
PalliatMed31:99–101.
https://doi.
org/10.
1177/0269216316686258SphereProject(2011a)Glossary:humanitarianaction.
http://www.
sphereproject.
org/handbook/glossary/l=H.
Accessed13Mar2018SphereProject(2011b)Humanitariancharter.
http://www.
spherehandbook.
org/en/the-humanitarian-charter/.
Accessed13Mar2018SphereProject(2017)Draft2oftheSphereHandbooknowreadyforreviewandfeedback.
http://www.
sphereproject.
org/handbook/revision-sphere-handbook/draft-ready-for-feedback/.
Accessed19Mar2018TerryF(2002)CondemnedtorepeatTheparadoxofhumanitarianaction.
CornellUniversityPress,IthacaThorneS(2016)Interpretivedescription:qualitativeresearchforappliedpractice,vol2.
Routledge,NewYorkThorneS,KirkhamSR,O'Flynn-MageeK(2004)Theanalyticchallengeininterpretivedescription.
IntJQualMethods3(1):1–11WebsterGC,BaylisFE(2000)Moralresidue.
In:RubinSB,ZolothL(eds)Marginoferror:theethicsofmistakesinthepracticeofmedicine.
UniversityPublishingGroup,Hagerstown,pp217–230WHO(2018)WHOmediacentrefactsheetonpalliativecare.
WorldHealthOrganization.
http://www.
who.
int/mediacentre/factsheets/fs402/en/.
Accessed20June2018Huntetal.
JournalofInternationalHumanitarianAction(2018)3:12Page13of13
阿里云年中活动最后一周 - ECS共享型N4 2G1M年付59元
以前我们在参与到云服务商促销活动的时候周期基本是一周时间,而如今我们会看到无论是云服务商还是电商活动基本上周期都要有超过一个月,所以我们有一些网友习惯在活动结束之前看看商家是不是有最后的促销活动吸引力的,比如有看到阿里云年中活动最后一周,如果我们有需要云服务器的可以看看。在前面的文章中(阿里云新人福利选择共享性N4云服务器年79.86元且送2月数据库),(LAOZUO.ORG)有提到阿里云今年的云...

spinservers:圣何塞10Gbps带宽服务器月付$109起,可升级1Gbps无限流量
spinservers是Majestic Hosting Solutions LLC旗下站点,主营国外服务器租用和Hybrid Dedicated等,数据中心在美国达拉斯和圣何塞机房。目前,商家针对圣何塞部分独立服务器进行促销优惠,使用优惠码后Dual Intel Xeon E5-2650L V3(24核48线程)+64GB内存服务器每月仅109美元起,提供10Gbps端口带宽,可以升级至1Gbp...

BuyVM商家4个机房的官方测试IP地址和测速文件
BuyVM 商家算是有一些年头,从早年提供低价便宜VPS主机深受广大网友抢购且也遭到吐槽的是因为审核账户太过于严格。毕竟我们国内的个人注册账户喜欢账户资料乱写,毕竟我们看英文信息有些还是比较难以识别的,于是就注册信息的时候随便打一些字符,这些是不能通过的。前几天,我们可以看到BUYVM商家有新增加迈阿密机房,而且商家有提供大硬盘且不限制流量的VPS主机,深受有一些网友的喜欢。目前,BUYVM商家有...
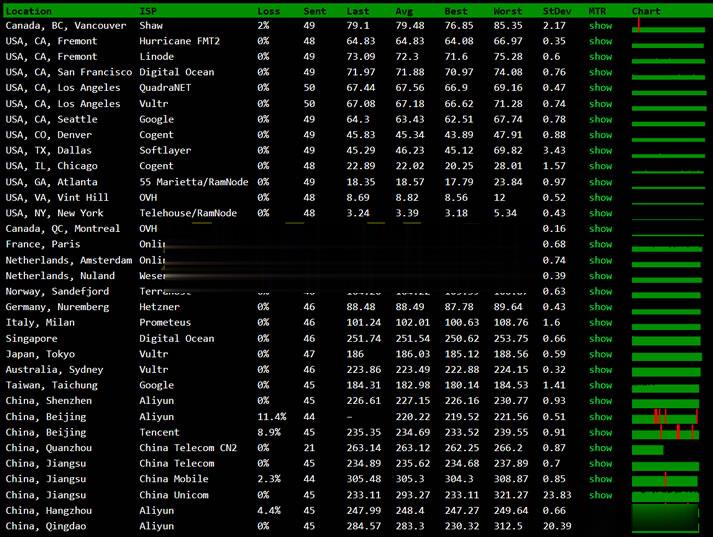
sonya为你推荐
-
域名域名的概念是什么?海外服务器租用外国服务器怎么租用?美国vps主机美国VPS好?还是香港VPS好?美国vps租用如何租用到最快的美国服务器美国服务器托管美国服务器租用时要注意什么?虚拟主机软件虚拟主机管理软件那个最好用?美国虚拟主机购买我公司需要购买美国的虚拟主机。但是为什么有的海外主机很便宜!有的却很贵呢。 质量如何区分!有没办法去四川虚拟主机222.214.218.100 请问这个IP是哪个服务商提供的?华众虚拟主机管理系统华众虚拟主机管理系统请问。华众 虚拟主机管理系统 这个问题 怎么解决 。就是后台可以开通虚拟主机 没有问题,但是 删除虚拟主机 后台显示删除成功的,但是实际在服务器上 文件夹 ftp iis站点 都没有被删除 是什么问题www二级域名一级域名和二级域名如何区别?例如,www.,加上了,yutian168.com,就是一级域名吗?